

Antiviral activity and safety of remdesivir against SARS-CoV-2 infection in human pluripotent stem cell-derived cardiomyocytes
- PMID: 33091434
- PMCID: PMC7571425
- DOI: 10.1016/j.antiviral.2020.104955
Antiviral activity and safety of remdesivir against SARS-CoV-2 infection in human pluripotent stem cell-derived cardiomyocytes
Abstract
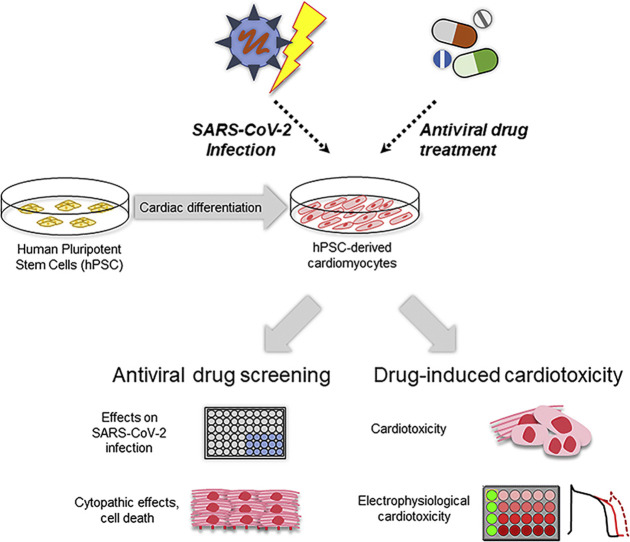
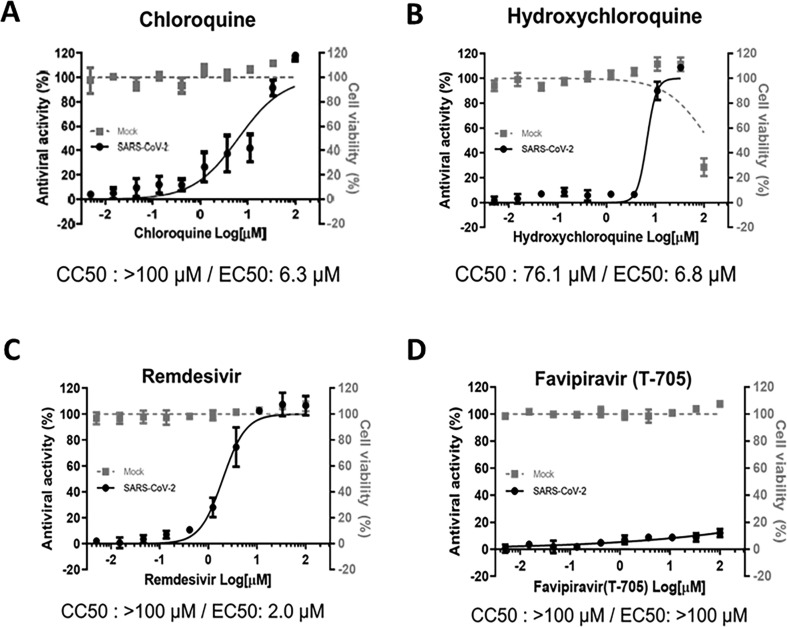
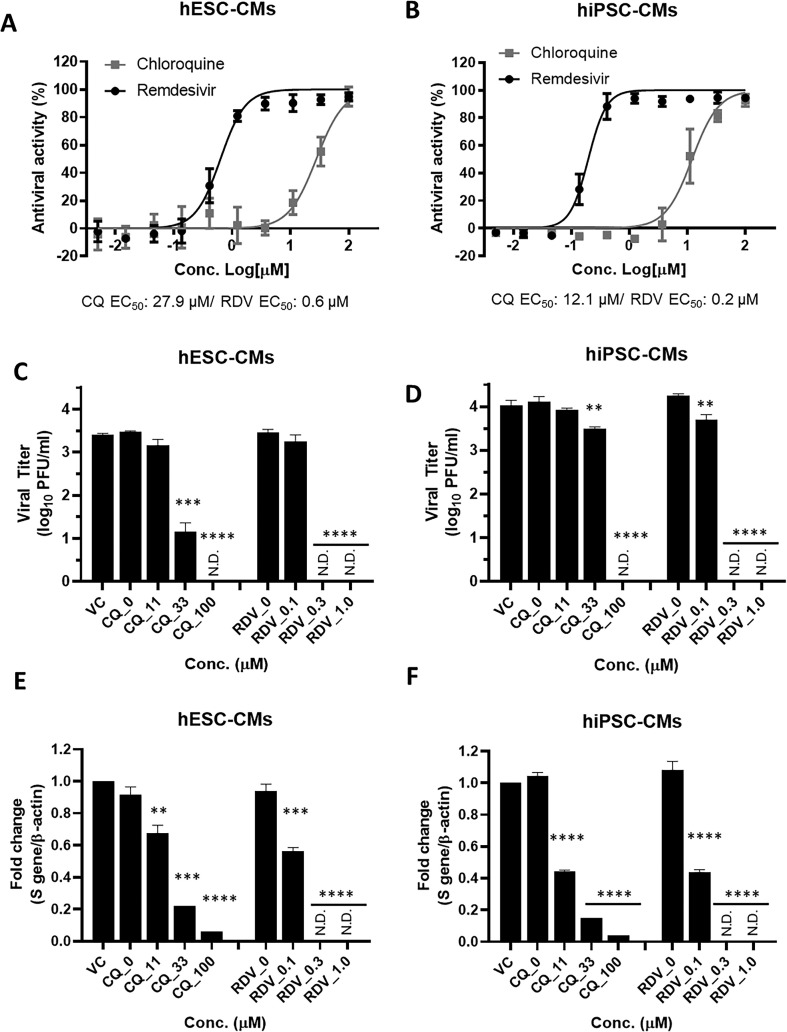
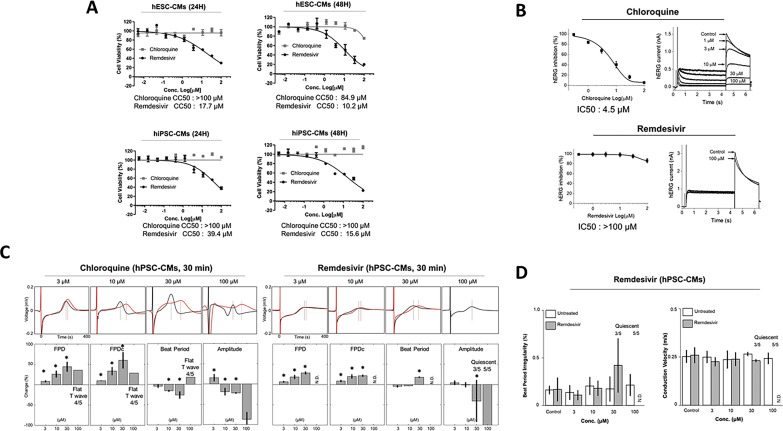
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), is considered as the most significant global public health crisis of the century. Several drug candidates have been suggested as potential therapeutic options for COVID-19, including remdesivir, currently the only authorized drug for use under an Emergency Use Authorization. However, there is only limited information regarding the safety profiles of the proposed drugs, in particular drug-induced cardiotoxicity. Here, we evaluated the antiviral activity and cardiotoxicity of remdesivir using cardiomyocytes-derived from human pluripotent stem cells (hPSC-CMs) as an alternative source of human primary cardiomyocytes (CMs). In this study, remdesivir exhibited up to 60-fold higher antiviral activity in hPSC-CMs compared to Vero E6 cells; however, it also induced moderate cardiotoxicity in these cells. To gain further insight into the drug-induced arrhythmogenic risk, we assessed QT interval prolongation and automaticity of remdesivir-treated hPSC-CMs using a multielectrode array (MEA). As a result, the data indicated a potential risk of QT prolongation when remdesivir is used at concentrations higher than the estimated peak plasma concentration. Therefore, we conclude that close monitoring of the electrocardiographic/QT interval should be advised in SARS-CoV-2-infected patients under remdesivir medication, in particular individuals with pre-existing heart conditions.
Keywords: COVID-19; Human cardiomyocytes; Pluripotent stem cells; Remdesivir; SARS-CoV-2.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Agency E.M. 2020. Summary on Compassionate Use: Remdesivir Gilead.https://www.ema.europa.eu/en/documents/other/summary-compassionate-use-r...
-
- Bojkova D., Wagner J.U.G., Shumliakivska M., Aslan G.S., Saleem U., Hansen A., Luxan G., Gunther S., Pham M.D., Krishnan J., Harter P.N., Ermel U.H., Frangakis A.S., Milting H., Zeiher A.M., Klingel K., Cinatl J., Dendorfer A., Eschenhagen T., Tschope C., Ciesek S., Dimmeler S. SARS-CoV-2 infects and induces cytotoxic effects in human cardiomyocytes. Cardiovasc. Res. 2020 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
