

Analyses of hemodialysis arteriovenous fistula geometric configuration and its associations with maturation and reintervention
- PMID: 33091518
- PMCID: PMC8055729
- DOI: 10.1016/j.jvs.2020.09.033
Analyses of hemodialysis arteriovenous fistula geometric configuration and its associations with maturation and reintervention
Abstract
Objective: An arteriovenous fistula (AVF) is the preferred vascular access for chronic hemodialysis; however, the rates of AVF maturation failure and reintervention remain high. We investigated the AVF geometric parameters and their associations with AVF physiologic maturation and reintervention in a prospective multicenter study.
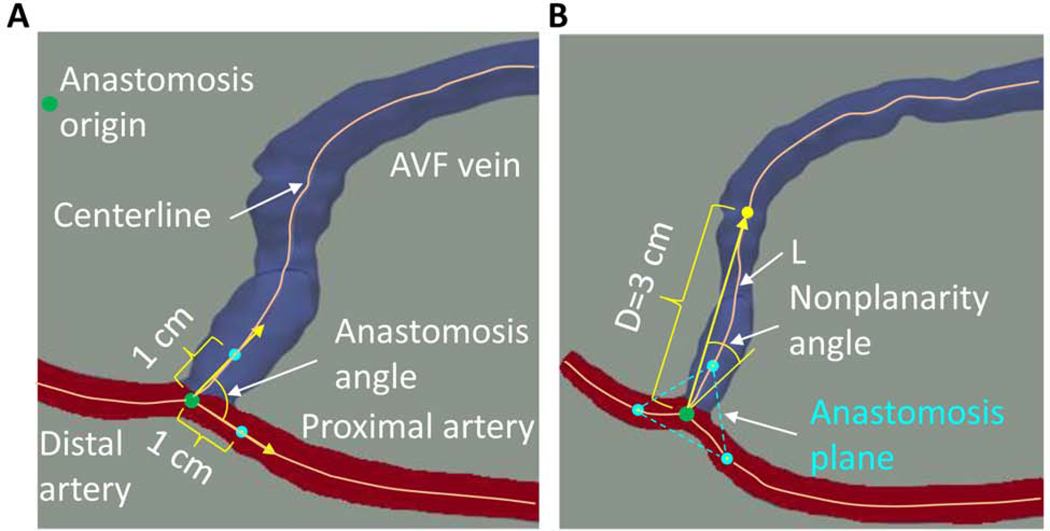
Methods: From 2011 to 2016, patients undergoing vein end-to-artery side upper extremity AVF creation surgery were recruited. Contrast-free dark blood and phase-contrast magnetic resonance imaging (MRI) scans were performed using 3.0T scanners to obtain the AVF lumen geometry and flow rates, respectively, at postoperative day 1, week 6, and month 6. The arteriovenous anastomosis angle, nonplanarity, and tortuosity of the fistula were calculated according to the lumen centerlines. AVFs were considered physiologically matured if, using the week 6 MRI data, the flow rate was ≥500 mL/min and the minimum vein lumen diameter was ≥5 mm. The associations of these geometric parameters with AVF maturation and reintervention due to perianastomotic and mid-vein stenosis within 1 year were assessed.
Results: A total of 111 patients had a usable day 1 MRI scan, with most having upper arm AVFs (n = 73). Compared with the forearm AVFs, upper arm AVFs had greater anastomosis angles (P < .001), larger deviations from a plane (nonplanarity; P = .002), and more prominent tortuosity (P = .038) at day 1. These parameters significantly increased between day 1 and week 6 in upper arm AVFs. In contrast, significant changes in these parameters in forearm AVFs were not observed. The rate of maturation was 54% and 86% for forearm and upper arm AVFs, respectively. None of the geometric parameters at day 1 were associated with AVF maturation in either location. The rate of reintervention was 24% and 30% for forearm and upper arm AVFs, respectively, with a larger nonplanarity angle at day 1 associated with less reintervention (30° ± 15° vs 21° ± 10°; P = .034) in upper arm AVFs only. This relationship was unchanged after adjusting for age, sex, race, dialysis status, or diabetes.
Conclusions: In our study, upper arm fistulas had a larger anastomosis angle, were more nonplanar, and had more tortuous veins than forearm fistulas. For upper arm fistulas, a larger nonplanarity angle is associated with a lower rate of reintervention within 1 year. Once confirmed, vascular surgeons could consider increasing the nonplanarity angle by incorporating a tension-free gentle curvature in the proximal segment of the mobilized vein to reduce reinterventions when creating an upper arm fistula.
Keywords: Anastomosis angle; Fistula maturation; Fistula stenosis; Hemodialysis arteriovenous fistula; Nonplanarity angle.
Copyright © 2020 Society for Vascular Surgery. All rights reserved.
Figures

References
-
- Lok CE, Huber TS, Lee T, Shenoy S, Yevzlin AS, Abreo K, et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am J Kidney Dis 2020;75:S1–S164. - PubMed
-
- Cunnane CV, Cunnane EM, Walsh MT. A review of the hemodynamic factors believed to contribute to vascular access dysfunction. Cardiovasc Eng Technol 2017;8:280–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
