

Serum Amyloid A in lung transplantation
- PMID: 33093763
- PMCID: PMC7569538
- DOI: 10.36141/svdld.v37i1.8775
Serum Amyloid A in lung transplantation
Abstract
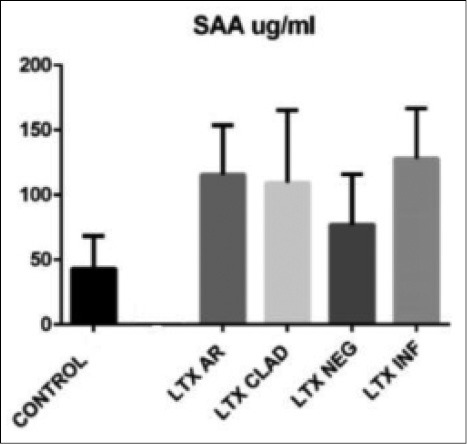
Background: Serum Amyloid A (SAA) is an acute phase protein and we analyzed its concentrations in lung transplantated patients (LTX).
Methods: 26 LTX patients (58.6 ± 11 years) and 11 healthy controls (55 ± 11.3 years). Three groups of LTX patients: acute rejection (AR, 7) bronchiolitis obliterans syndrome (BOS, 3), acute infection (INF, 9) and stable patients (NEG, 7).
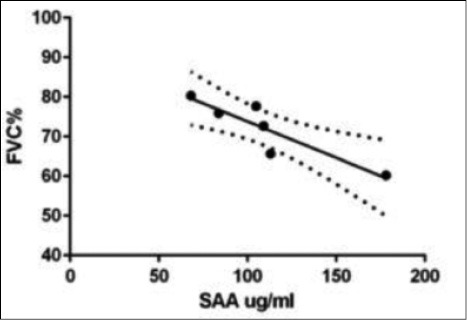
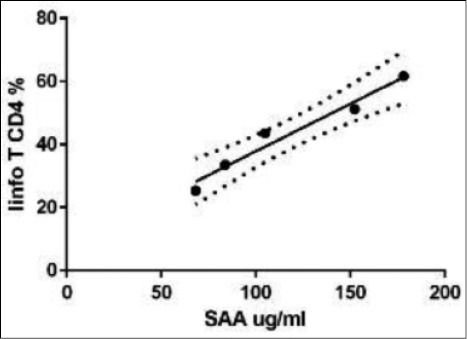
Results: In LTX patients SAA concentrations were significantly increased, particularly in AR and INF. In LTX-AR patients were observed a correlation between SAA levels and peripheral CD4+ lymphocyte percentage (r=0.9, p<0.01) and a reverse correlation with FVC percentages (r -0.94, p=0.01).
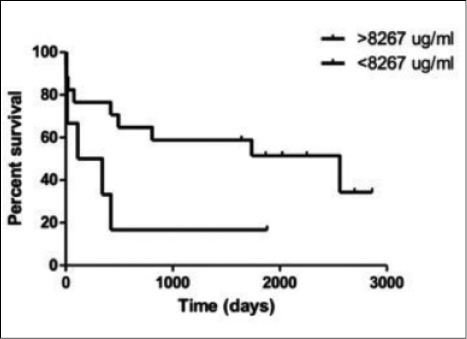
Conclusions: SAA may represent a potential biomarker of LTX acute complications, with a prognostic value in AR. (Sarcoidosis Vasc Diffuse Lung Dis 2020; 37 (1): 2-7).
Keywords: lung transplantation; serum amyloid A; serum biomarkers.
Copyright: © 2020 SARCOIDOSIS VASCULITIS AND DIFFUSE LUNG DISEASES.
Figures
References
-
- Christie JD, Edwards LB, Aurora P, et al. Registry of the international Society for heart and lung tranplantation: twenty-fifth official adult lung and heart-lung transplantation report 2008. J Heart Lung Transplant. 2008;27:957–969. - PubMed
-
- Egan TM, Murray S, Bustami RT, et al. Development of the new Lung Allocation System in the Unisted States. Am J Trasplant. 2006;6:1212–1227. - PubMed
-
- Stewart S, et al. Revision of the 1996 working formulation for the standardization of nomenclature in the diagnosis of heart and lung rejection. J Heart Lung Transplant. 2007:1229–1242. - PubMed
-
- Yousen SA. Lymphocytic bronchitis/bronchiolitis in lung allograft recipients. Am J Surg Pathol. 1993;17:491–496. - PubMed
-
- Boehler A, Estenne M. Post-transplant bronchiolitis obliterans. Eur Respir J. 2003;22:1007–1018. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials