

Next-generation sequencing-guided molecular-targeted therapy and immunotherapy for biliary tract cancers
- PMID: 33095329
- PMCID: PMC10992508
- DOI: 10.1007/s00262-020-02745-y
Next-generation sequencing-guided molecular-targeted therapy and immunotherapy for biliary tract cancers
Abstract
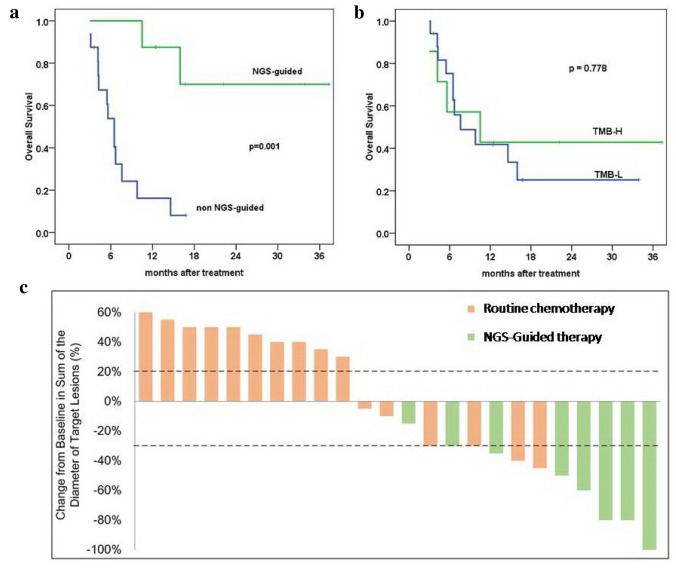
Background: Chemotherapy is a standard regimen for advanced or relapsed biliary tract cancer (BTC) with a 5-year overall survival (OS) rate of approximately 5% and a median OS of less than a year. Targeted therapies and immunotherapy aimed at providing more personalized treatments for BTCs have been tested. The objective of this study was to evaluate the effects of targeted therapy and immunotherapy on advanced BTC patients.
Methods: Twenty-four advanced/relapsed BTC patients were enrolled and examined with next-generation sequencing (NGS). Eight of them received NGS-guided targeted or immunotherapy, and the other 16 patients underwent routine chemotherapy. Comparison analysis of OS and objective response rate (ORR) was performed.
Results: IDH1, BRCA2, MAP2K1, and BRAF (V600E) were the major actionable genes mutated in this cohort. Patients who received NGS-guided therapy exhibited higher OS (not achieved vs. 6.5 months, p < 0.001) and ORR (87.5% vs. 25%, p < 0.001) than those without targetable mutations and who received first-line chemotherapy. BTCs harboring mutations in IDH1, ATM/BRCA2, or MAP2K1/BRAF (V600E) received treatment with dasatinib, olaparib, or trametinib, respectively. Three of the patients had high tumor mutation burden (TMB-H) and were treated with immune-checkpoint inhibitors and chemotherapy. All these patients achieved complete response or partial response.
Conclusions: NGS-guided targeted therapy and immunotherapy are promising personalized therapies for advanced or relapsed BTCs. TMB is a useful biomarker for predicting immunotherapy efficacy.
Keywords: Biliary tract cancer; Immunotherapy; Next-generation sequencing; Personalized medicine; Targeted therapy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




Similar articles
-
Targeted deep sequencing contributes to guiding personalized targeted therapy for advanced biliary tract cancer patients with non‑radical resection: A real‑world study.Oncol Rep. 2020 Apr;43(4):1089-1102. doi: 10.3892/or.2020.7491. Epub 2020 Feb 6. Oncol Rep. 2020. PMID: 32323774 Free PMC article.
-
Dabrafenib plus trametinib in patients with BRAFV600E-mutated biliary tract cancer (ROAR): a phase 2, open-label, single-arm, multicentre basket trial.Lancet Oncol. 2020 Sep;21(9):1234-1243. doi: 10.1016/S1470-2045(20)30321-1. Epub 2020 Aug 17. Lancet Oncol. 2020. PMID: 32818466 Clinical Trial.
-
Therapeutic relevance of targeted sequencing in management of patients with advanced biliary tract cancer: DNA damage repair gene mutations as a predictive biomarker.Eur J Cancer. 2019 Oct;120:31-39. doi: 10.1016/j.ejca.2019.07.022. Epub 2019 Aug 30. Eur J Cancer. 2019. PMID: 31476489
-
Systemic treatment of advanced or recurrent biliary tract cancer.Biosci Trends. 2020 Nov 4;14(5):328-341. doi: 10.5582/bst.2020.03240. Epub 2020 Aug 24. Biosci Trends. 2020. PMID: 32830166 Review.
-
The choice for the optimal therapy in advanced biliary tract cancers: Chemotherapy, targeted therapies or immunotherapy.Pharmacol Ther. 2020 Jun;210:107517. doi: 10.1016/j.pharmthera.2020.107517. Epub 2020 Feb 25. Pharmacol Ther. 2020. PMID: 32109491 Review.
Cited by
-
Systemic Treatment for Metastatic Biliary Tract Cancer: State of the Art and a Glimpse to the Future.Curr Oncol. 2022 Jan 27;29(2):551-564. doi: 10.3390/curroncol29020050. Curr Oncol. 2022. PMID: 35200550 Free PMC article. Review.
-
Mutational spectrum for guiding the decision of adjuvant treatment in patients with resected biliary tract carcinoma.Cancer Med. 2023 Aug;12(15):16076-16086. doi: 10.1002/cam4.6261. Epub 2023 Jun 21. Cancer Med. 2023. PMID: 37341068 Free PMC article.
-
Combined Immunotherapy and Targeted Therapies for Cancer Treatment: Recent Advances and Future Perspectives.Curr Cancer Drug Targets. 2023;23(4):251-264. doi: 10.2174/1568009623666221020104603. Curr Cancer Drug Targets. 2023. PMID: 36278447 Review.
-
Molecular Landscape and Therapeutic Strategies in Cholangiocarcinoma: An Integrated Translational Approach towards Precision Medicine.Int J Mol Sci. 2021 May 25;22(11):5613. doi: 10.3390/ijms22115613. Int J Mol Sci. 2021. PMID: 34070643 Free PMC article. Review.
-
Adjuvant therapy for intrahepatic carcinoma after surgical resection: chemotherapy and future perspectives.Hepatobiliary Surg Nutr. 2021 Dec;10(6):878-880. doi: 10.21037/hbsn-21-368. Hepatobiliary Surg Nutr. 2021. PMID: 35004960 Free PMC article. No abstract available.
References
MeSH terms
Substances
Grants and funding
- 81572434/National Natural Science Foundation of China
- 2018ZX10723204-007-001/Ministry of Science and Technology, National Science and Technology Major Special Project
- 2017-1-35/"Young Medical Elites," Tianjin Health Commission
- 2018-2-8/"Young Innovative Talents," Tianjin Medical University Cancer Institute and Hospital
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
