

Neuromuscular blocking agents in acute respiratory distress syndrome: updated systematic review and meta-analysis of randomized trials
- PMID: 33095344
- PMCID: PMC7582438
- DOI: 10.1186/s40635-020-00348-6
Neuromuscular blocking agents in acute respiratory distress syndrome: updated systematic review and meta-analysis of randomized trials
Abstract
Purpose: Existing clinical practice guidelines support the use of neuromuscular blocking agents (NMBA) in acute respiratory distress syndrome (ARDS); however, a recent large randomized clinical trial (RCT) has questioned this practice. Therefore, we updated a previous systematic review to determine the efficacy and safety of NMBAs in ARDS.
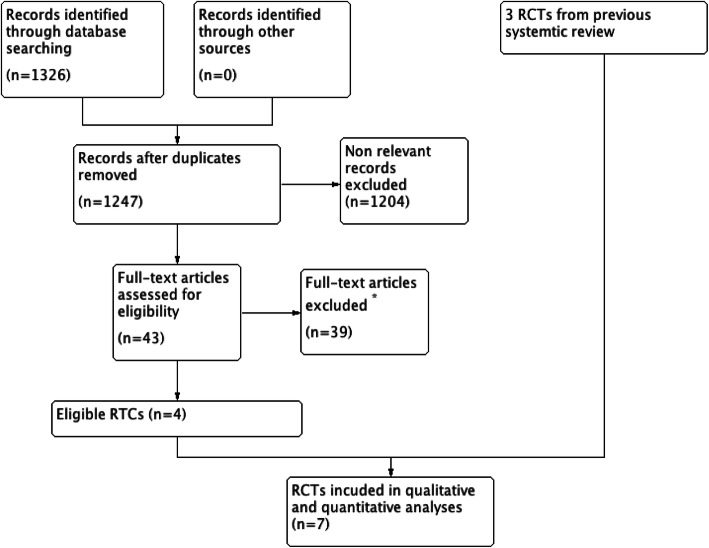
Methods: We searched MEDLINE, EMBASE (October 2012 to July 2019), the Cochrane (Central) database, and clinical trial registries ( ClinicalTrials.gov , ISRCTN Register, and WHO ICTRP) for RCTs comparing the effects of NMBA as a continuous infusion versus placebo or no NMBA infusion (but allowing intermittent NMBA boluses) on patient-important outcomes for adults with ARDS. Two independent reviewers assessed the methodologic quality of the primary studies and abstracted data.
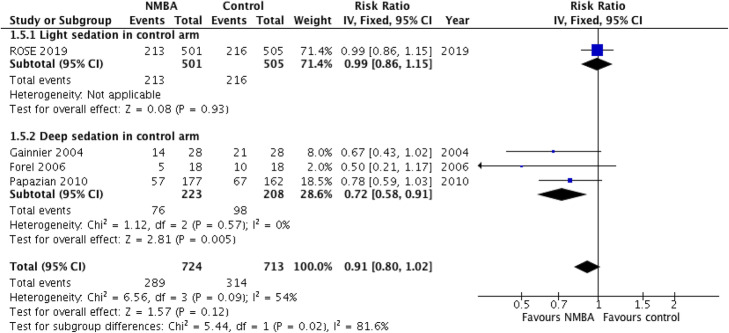
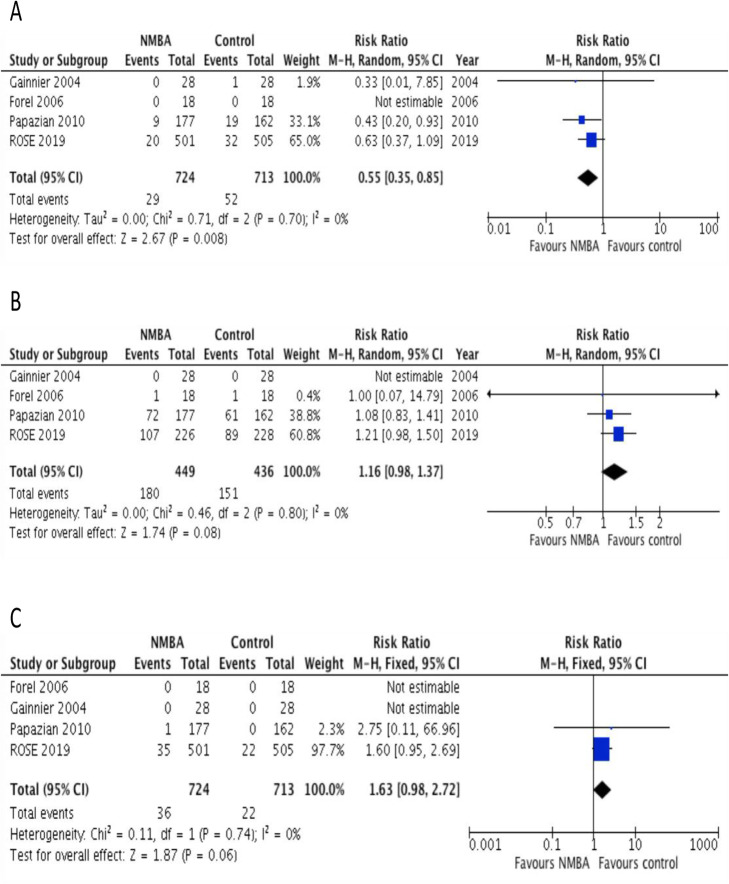
Results: Seven RCTs, including four new RCTs, met eligibility criteria for this review. These trials enrolled 1598 patients with moderate to severe ARDS at centers in the USA, France, and China. All trials assessed short-term continuous infusions of cisatracurium or vecuronium. The pooled estimate for mortality outcomes showed significant statistical heterogeneity, which was only explained by a subgroup analysis by depth of sedation in the control arm. A continuous NMBA infusion did not improve mortality when compared to a light sedation strategy with no NMBA infusion (relative risk [RR] 0.99; 95% CI 0.86-1.15; moderate certainty; P = 0.93). On the other hand, continuous NMBA infusion reduced mortality when compared to deep sedation with as needed NMBA boluses (RR 0.71; 95% CI 0.57-0.89; low certainty; P = 0.003). Continuous NMBA infusion reduced the rate of barotrauma (RR 0.55; 95% CI 0.35-0.85, moderate certainty; P = 0.008) across eligible trials, but the effect on ventilator-free days, duration of mechanical ventilation, and ICU-acquired weakness was uncertain.
Conclusions: Inconsistency in study methods and findings precluded the pooling of all trials for mortality. In a pre-planned sensitivity analysis, the impact of NMBA infusion on mortality depends on the strategy used in the control arm, showing reduced mortality when compared to deep sedation, but no effect on mortality when compared to lighter sedation. In both situations, a continuous NMBA infusion may reduce the risk of barotrauma, but the effects on other patient-important outcomes remain unclear. Future research, including an individual patient data meta-analysis, could help clarify some of the observed findings in this updated systematic review.
Keywords: ARDS; Neuromuscular blockade; Systematic review.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, DF MA, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, Investigators LS. Group ET Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Herridge MS, Tansey CM, Matte A, Tomlinson G, Diaz-Granados N, Cooper A, Guest CB, Mazer CD, Mehta S, Stewart TE, Kudlow P, Cook D, Slutsky AS, Cheung AM, Canadian Critical Care Trials G Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364:1293–1304. doi: 10.1056/NEJMoa1011802. - DOI - PubMed
-
- Acute Respiratory Distress Syndrome N. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
