

The Pathogenic Role of Demodex Mites in Rosacea: A Potential Therapeutic Target Already in Erythematotelangiectatic Rosacea?
- PMID: 33095403
- PMCID: PMC7649190
- DOI: 10.1007/s13555-020-00458-9
The Pathogenic Role of Demodex Mites in Rosacea: A Potential Therapeutic Target Already in Erythematotelangiectatic Rosacea?
Abstract
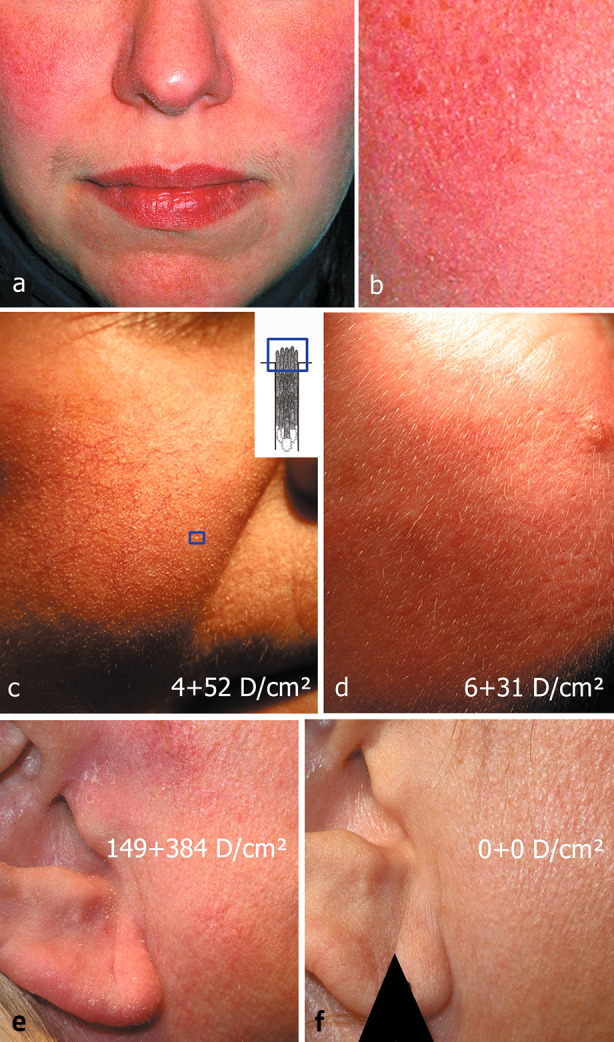
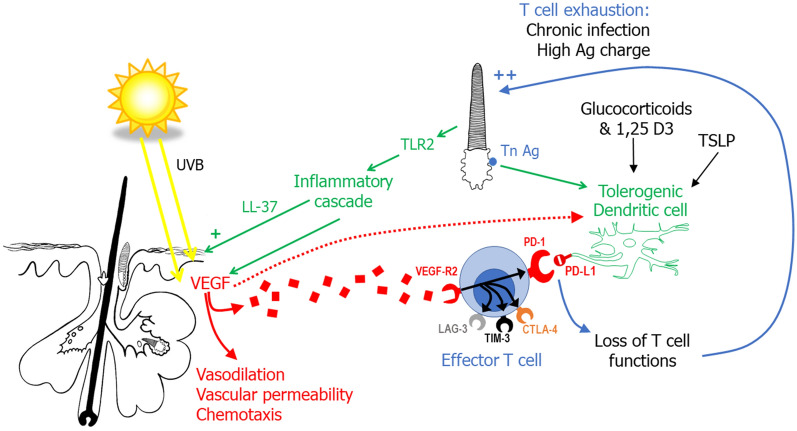
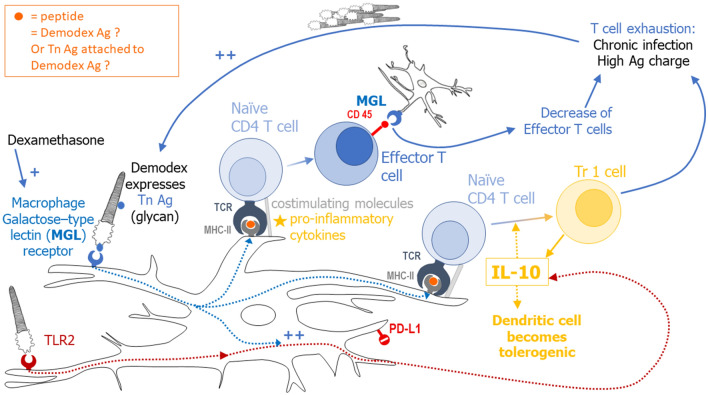
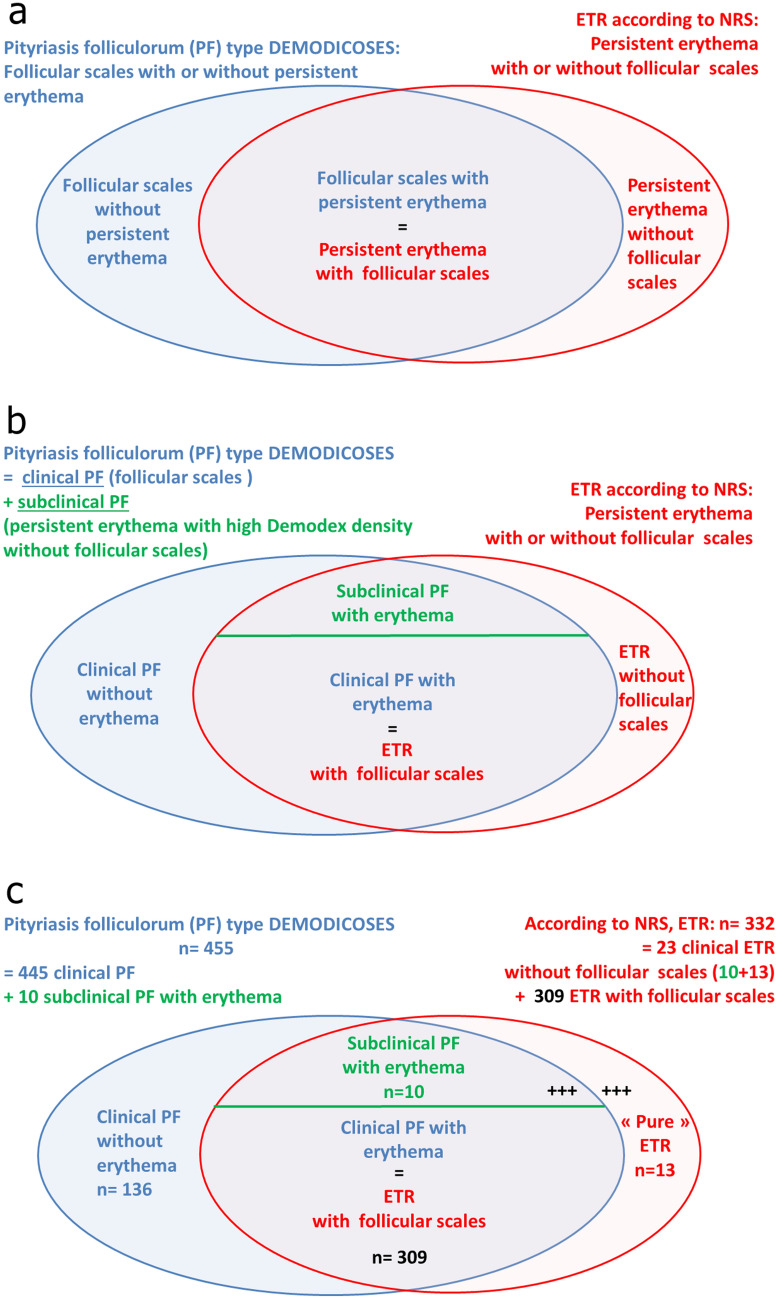
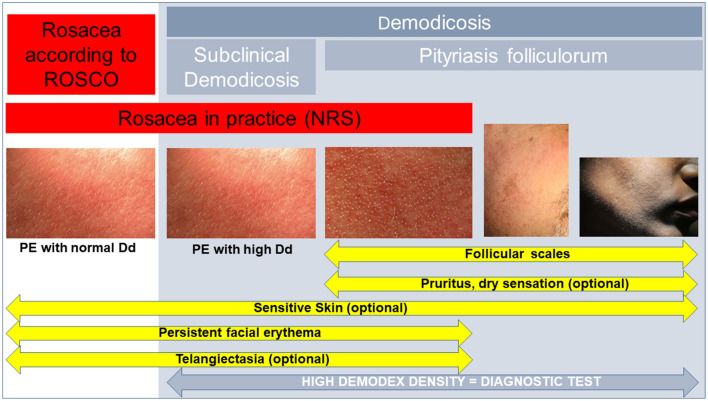
Rosacea is a common facial dermatosis but its definition and classification are still unclear, especially in terms of its links with demodicosis. Triggers of rosacea (ultraviolet light, heat, spicy foods, alcohol, stress, microbes) are currently considered to induce a cascading innate and then adaptive immune response that gets out of control. Recent histological and biochemical studies support the concept that this inflammatory response is a continuum, already present from the onset of the disease, even when no clinical signs of inflammation are visible. The Demodex mite is beginning to be accepted as one of the triggers of this inflammatory cascade, and its proliferation as a marker of rosacea; moreover, the papulopustules of rosacea can be effectively treated with topical acaricidal agents. Demodex proliferation appears to be a continuum process in rosacea, and may not be clinically visible at the onset of the disease. Molecular studies suggest that Demodex may induce tolerogenic dendritic cells and collaborate with vascular endothelial growth factor (VEGF) to induce T cell exhaustion and favor its own proliferation. These interactions among VEGF, Demodex, and immunity need to be explored further and the nosology of rosacea adapted accordingly. However, treating early rosacea, with only clinically visible vascular symptoms, with an acaricide may decrease early inflammation, limit potential flare-ups following laser treatment, and prevent the ultimate development of the papulopustules of rosacea. The effectiveness of this approach needs to be confirmed by prospective controlled clinical trials with long-term follow-up. Currently, the evidence suggests that patients with only vascular symptoms of rosacea should be carefully examined for the presence of follicular scales as signs of Demodex overgrowth or pityriasis folliculorum so that these patients, at least, can be treated early with an acaricidal cream.
Keywords: Benzyl benzoate; Demodicosis; Dendritic cell; Immunotolerance; Ivermectin; MGL; Rosacea; Standardized skin surface biopsy; Tn Ag; VEGF.
Figures
References
-
- Cribier B. Rosacée: nouveautés pour une meilleure prise en charge. Ann Dermatol Venereol. 2017;144:508–517. - PubMed
-
- Berg M, Lidén S. An epidemiological study of rosacea. Acta Derm Venereol. 1989;69:419–423. - PubMed
-
- Gether L, Overgaard LK, Egeberg A, Thyssen JP. Incidence and prevalence of rosacea: a systematic review and meta-analysis. Br J Dermatol. 2018;179:282–289. - PubMed
-
- Buddenkotte J, Steinhoff M. Recent advances in understanding and managing rosacea. F1000Res. 2018;7:F1000 Faculty Rev-1885.
Publication types
LinkOut - more resources
Full Text Sources
