

Chest CT in COVID-19: What the Radiologist Needs to Know
- PMID: 33095680
- PMCID: PMC7587296
- DOI: 10.1148/rg.2020200159
Chest CT in COVID-19: What the Radiologist Needs to Know
Erratum in
-
Chest CT in COVID-19: What the Radiologist Needs to Know.Radiographics. 2022 Jan-Feb;42(1):E32. doi: 10.1148/rg.219015. Radiographics. 2022. PMID: 34990334 Free PMC article. No abstract available.
Abstract
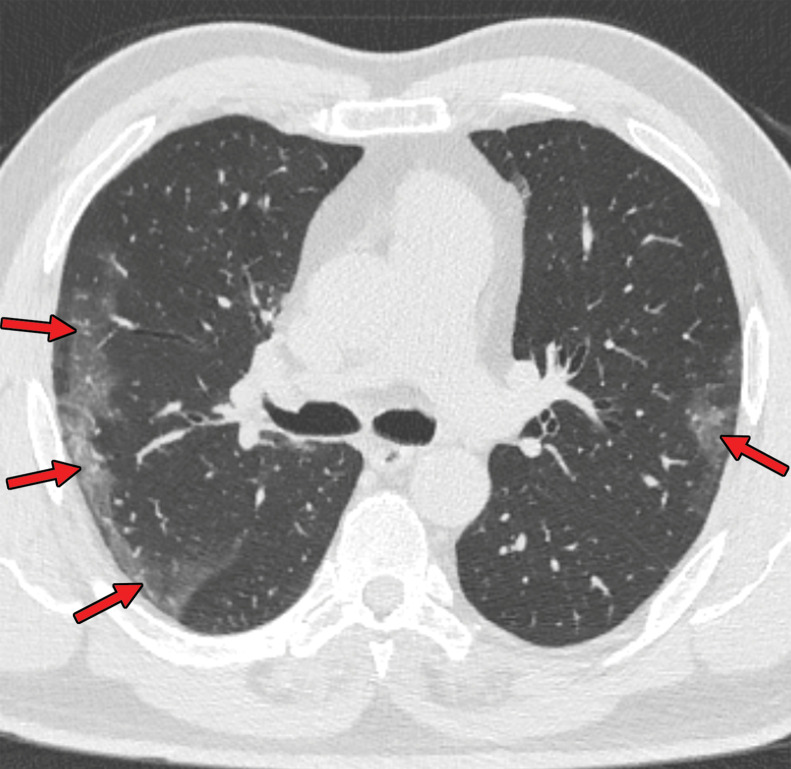
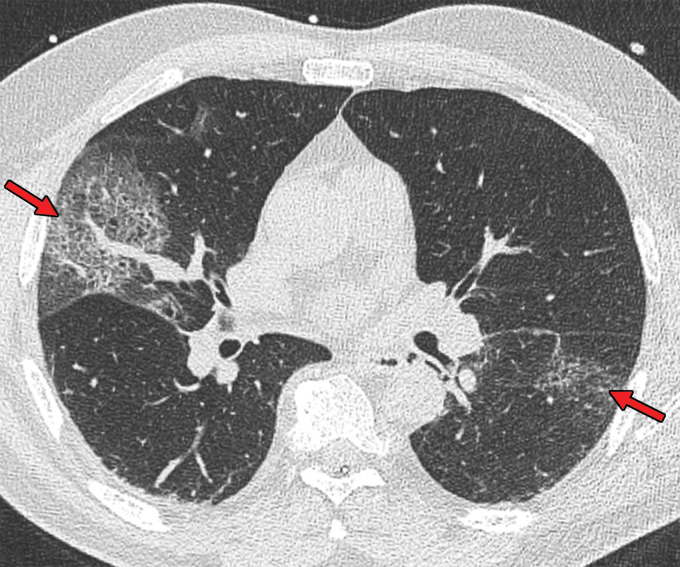
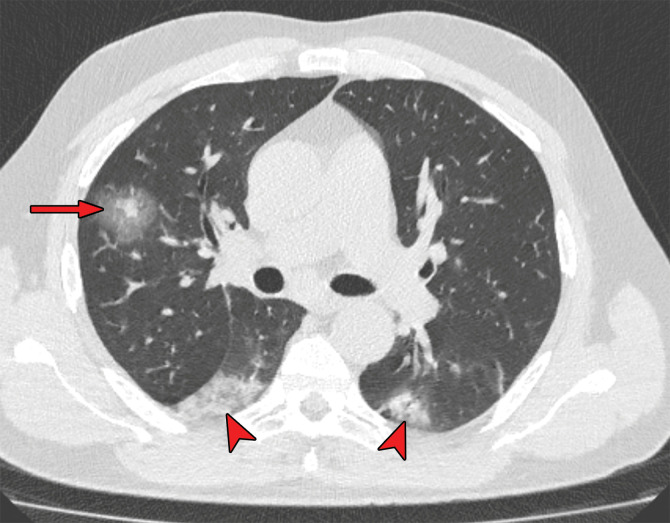
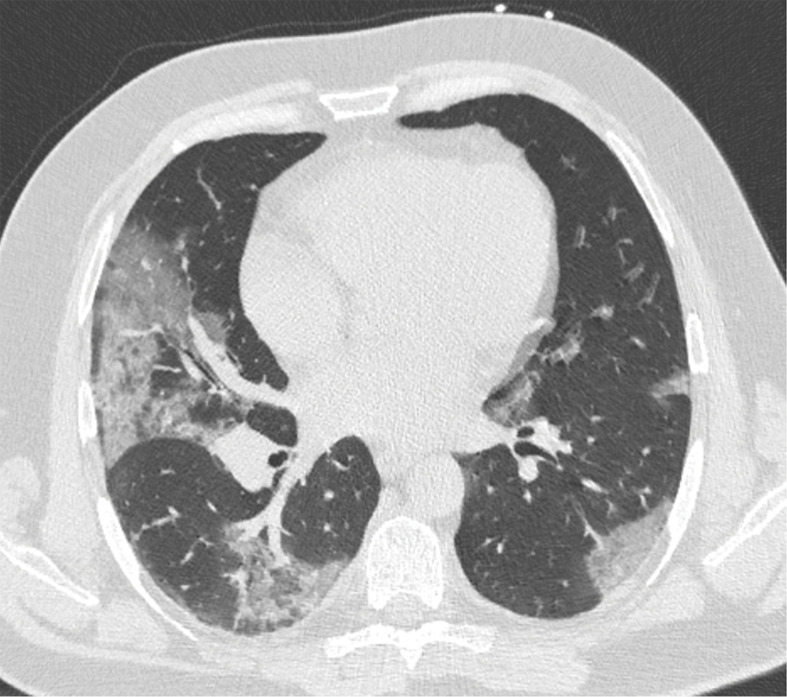
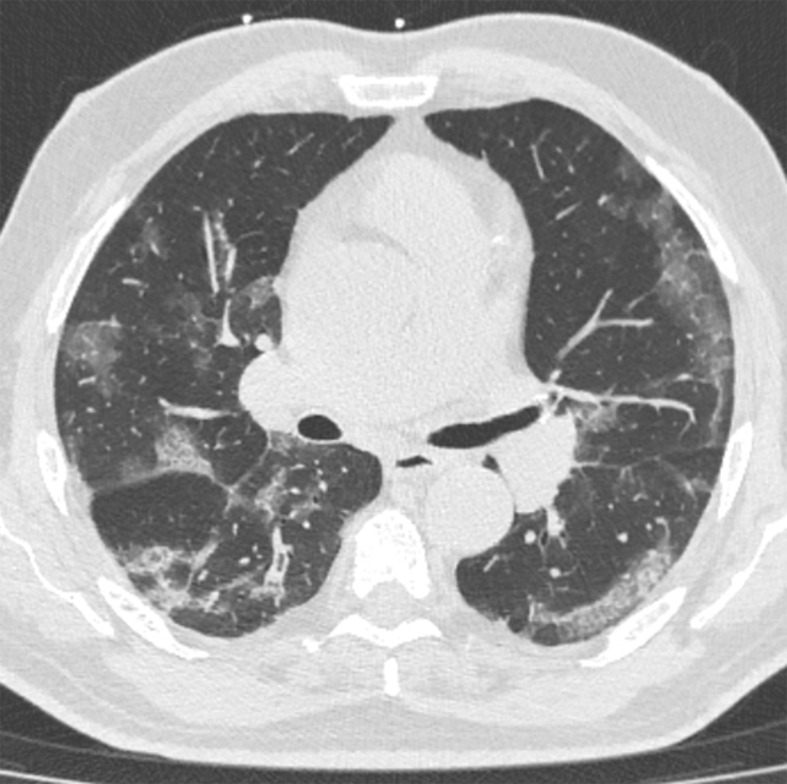
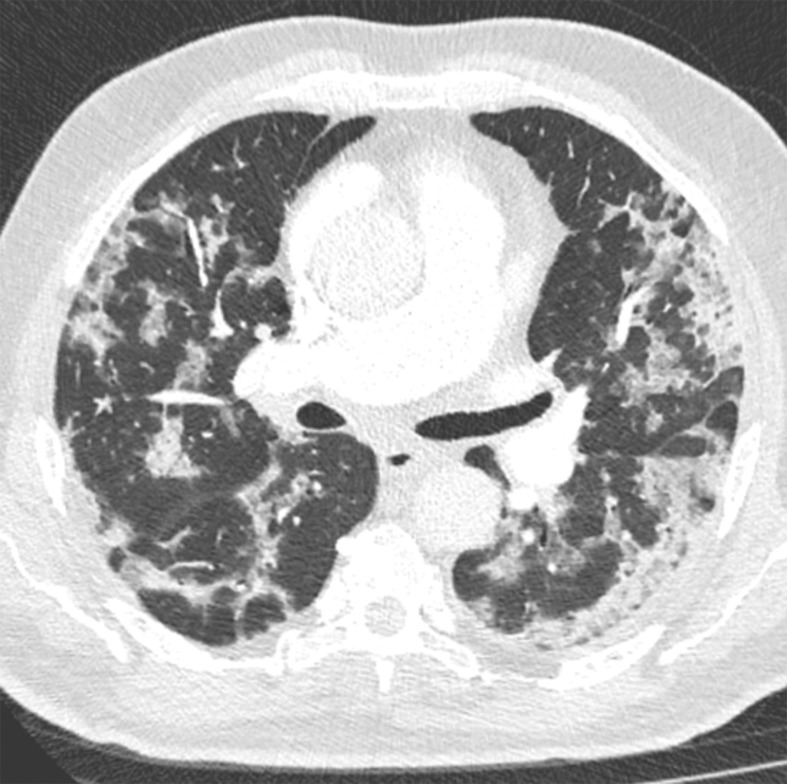
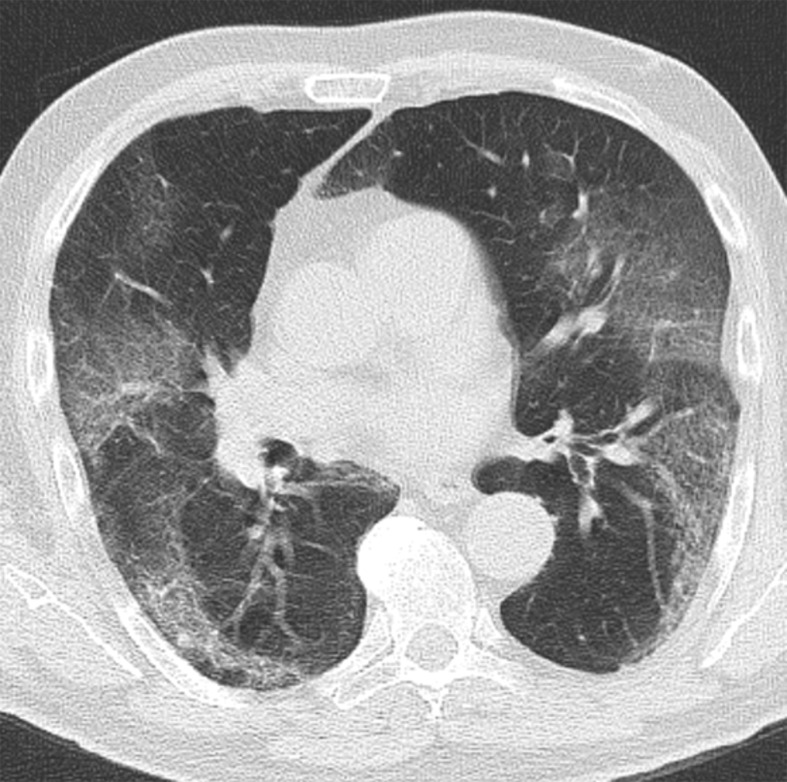
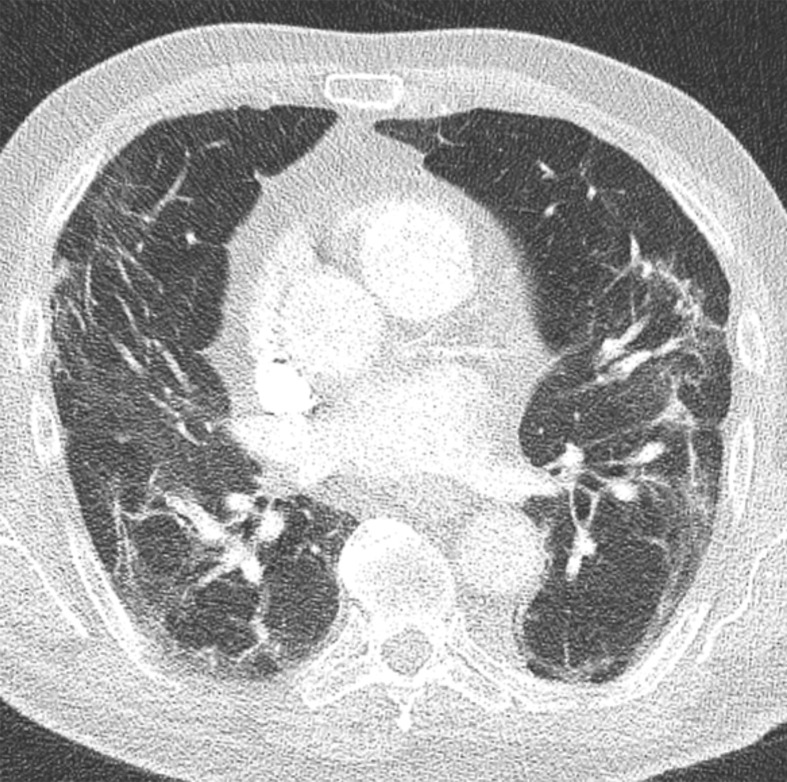
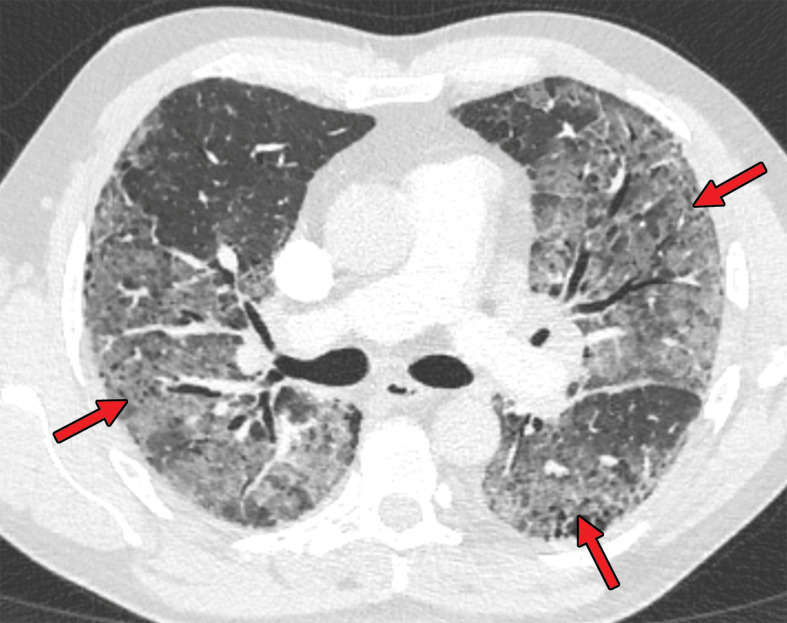
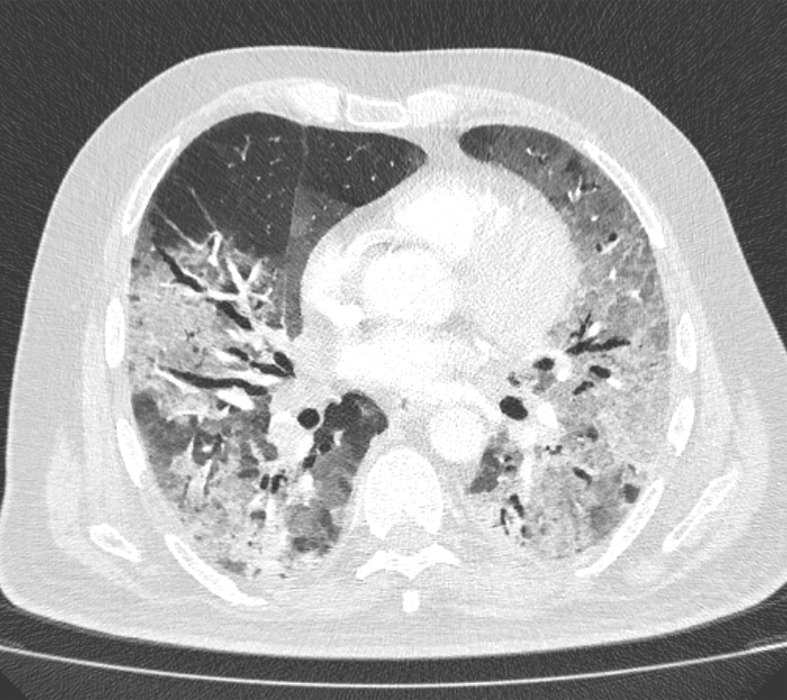
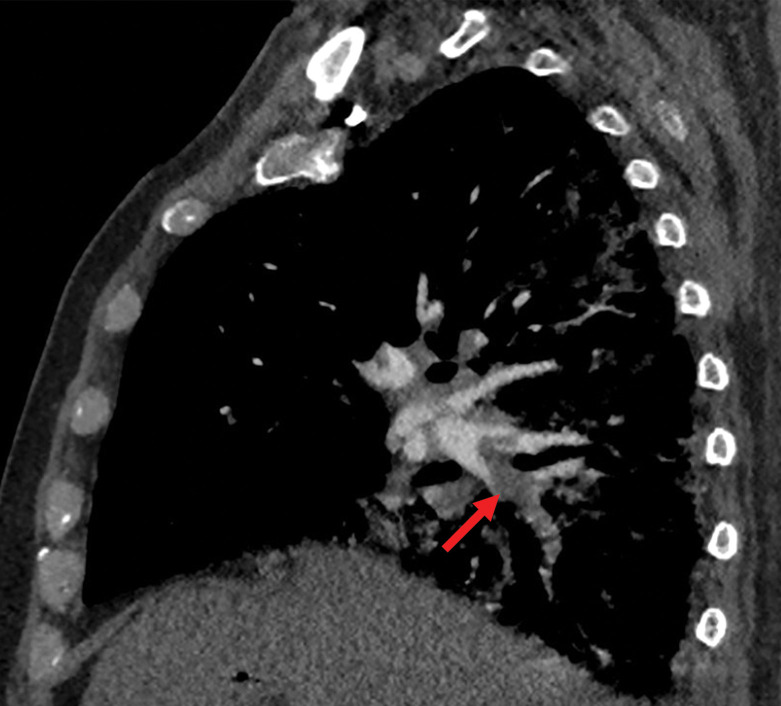
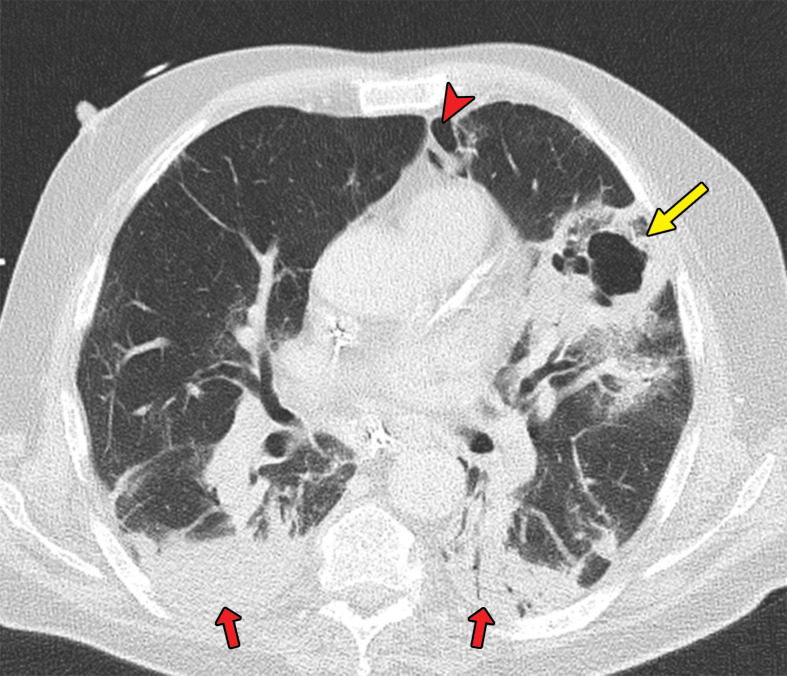
Chest CT has a potential role in the diagnosis, detection of complications, and prognostication of coronavirus disease 2019 (COVID-19). Implementation of appropriate precautionary safety measures, chest CT protocol optimization, and a standardized reporting system based on the pulmonary findings in this disease will enhance the clinical utility of chest CT. However, chest CT examinations may lead to both false-negative and false-positive results. Furthermore, the added value of chest CT in diagnostic decision making is dependent on several dynamic variables, most notably available resources (real-time reverse transcription-polymerase chain reaction [RT-PCR] tests, personal protective equipment, CT scanners, hospital and radiology personnel availability, and isolation room capacity) and the prevalence of both COVID-19 and other diseases with overlapping manifestations at chest CT. Chest CT is valuable to detect both alternative diagnoses and complications of COVID-19 (acute respiratory distress syndrome, pulmonary embolism, and heart failure), while its role for prognostication requires further investigation. The authors describe imaging and managing care of patients with COVID-19, with topics including (a) chest CT protocol, (b) chest CT findings of COVID-19 and its complications, (c) the diagnostic accuracy of chest CT and its role in diagnostic decision making and prognostication, and (d) reporting and communicating chest CT findings. The authors also review other specific topics, including the pathophysiology and clinical manifestations of COVID-19, the World Health Organization case definition, the value of performing RT-PCR tests, and the radiology department and personnel impact related to performing chest CT in COVID-19. ©RSNA, 2020.
Figures










Comment in
-
Chest CT in "Post" COVID-19: What the Radiologist Must Know.Radiographics. 2021 Mar-Apr;41(2):E66-E67. doi: 10.1148/rg.2021200213. Radiographics. 2021. PMID: 33646900 Free PMC article. No abstract available.
References
-
- World Health Organization . Coronavirus . https://www.who.int/health-topics/coronavirus#tab=tab_1 . Accessed June 6, 2020 .
-
- World Health Organization . Pneumonia of unknown caus: China . https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-ch... . Published January 5, 2020. Accessed June 6, 2020 .
-
- World Health Organization . WHO announces COVID-19 outbreak a pandemic . http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-... . Published March 12, 2020. Accessed June 6, 2020 .
-
- Johns Hopkins University School of Medicine . Coronavirus Resource Center . https://coronavirus.jhu.edu/ . Updated June 13, 2020. Accessed June 13, 2020 .
-
- Thanh Le T , Andreadakis Z , Kumar A , et al. The COVID-19 vaccine development landscape . Nat Rev Drug Discov 2020. ; 19 ( 5 ): 305 – 306 . - PubMed
