

White matter tract microstructure and cognitive performance after transient ischemic attack
- PMID: 33095770
- PMCID: PMC7584182
- DOI: 10.1371/journal.pone.0239116
White matter tract microstructure and cognitive performance after transient ischemic attack
Abstract
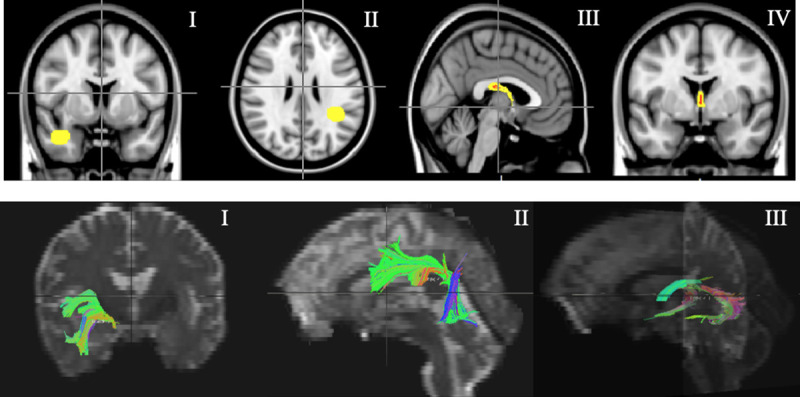
Background and purpose: Patients with transient ischemic attack (TIA) show evidence of cognitive impairment but the reason is not clear. Measurement of microstructural changes in white matter (WM) using diffusion tensor imaging (DTI) may be a useful outcome measure. We report WM changes using DTI and the relationship with neuropsychological performance in a cohort of transient ischemic attack (TIA) and non-TIA subjects.
Methods: Ninety-five TIA subjects and 51 non-TIA subjects were assessed using DTI and neuropsychological batteries. Fractional anisotropy (FA) and mean diffusivity (MD) maps were generated and measurements were collected from WM tracts. Adjusted mixed effects regression modelled the relationship between groups and DTI metrics.
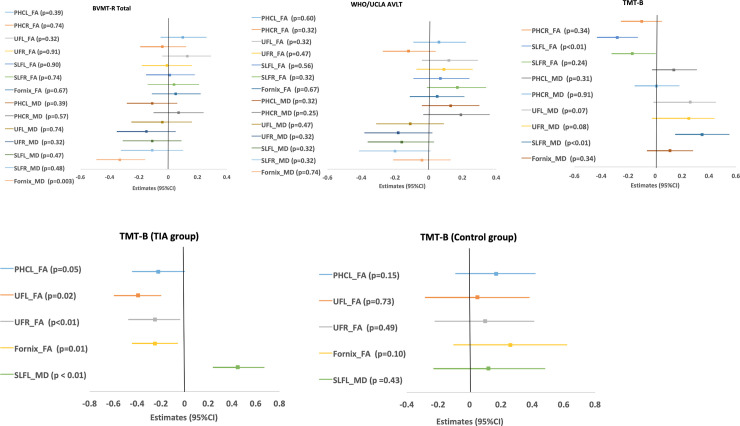
Results: Transient ischemic attack subjects had a mean age of 67.9 ± 9.4 years, and non-TIA subjects had a mean age 64.9 ± 9.9 years. The TIA group exhibited higher MD values in the fornix (0.36 units, P < 0.001) and lower FA in the superior longitudinal fasciculus (SLF) (-0.29 units, P = 0.001), genu (-0.22 units, P = 0.016), and uncinate fasciculus (UF) (-0.26 units, P = 0.004). Compared to non-TIA subjects, subjects with TIA scored lower on the Addenbrooke's Cognitive Assessment-Revised (median score 95 vs 91, P = 0.01) but showed no differences in scores on the Montreal Cognitive Assessment (median 27 vs 26) or the Mini-Mental State Examination (median 30). TIA subjects had lower scores in memory (median 44 vs 52, P < 0.01) and processing speed (median 45 vs 62, P < 0.01) but not executive function, when compared to non-TIA subjects. Lower FA and higher MD in the fornix, SLF, and UF were associated with poorer performance on tests of visual memory and executive function but not verbal memory. Lower FA in the UF and fornix were related to higher timed scores on the TMT-B (P < 0.01), and higher SLF MD was related to higher scores on TMT-B (P < 0.01), confirming worse executive performance in the TIA group.
Conclusions: DTI scans may be useful for detecting microstructural disease in TIA subjects before cognitive symptoms develop. DTI parameters, white matter hyperintensities, and vascular risk factors underly some of the altered neuropsychological measures in TIA subjects.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
