

Effect of Regional Citrate Anticoagulation vs Systemic Heparin Anticoagulation During Continuous Kidney Replacement Therapy on Dialysis Filter Life Span and Mortality Among Critically Ill Patients With Acute Kidney Injury: A Randomized Clinical Trial
- PMID: 33095849
- PMCID: PMC7585036
- DOI: 10.1001/jama.2020.18618
Effect of Regional Citrate Anticoagulation vs Systemic Heparin Anticoagulation During Continuous Kidney Replacement Therapy on Dialysis Filter Life Span and Mortality Among Critically Ill Patients With Acute Kidney Injury: A Randomized Clinical Trial
Abstract
Importance: Although current guidelines suggest the use of regional citrate anticoagulation (which involves the addition of a citrate solution to the blood before the filter of the extracorporeal dialysis circuit) as first-line treatment for continuous kidney replacement therapy in critically ill patients, the evidence for this recommendation is based on few clinical trials and meta-analyses.
Objective: To determine the effect of regional citrate anticoagulation, compared with systemic heparin anticoagulation, on filter life span and mortality.
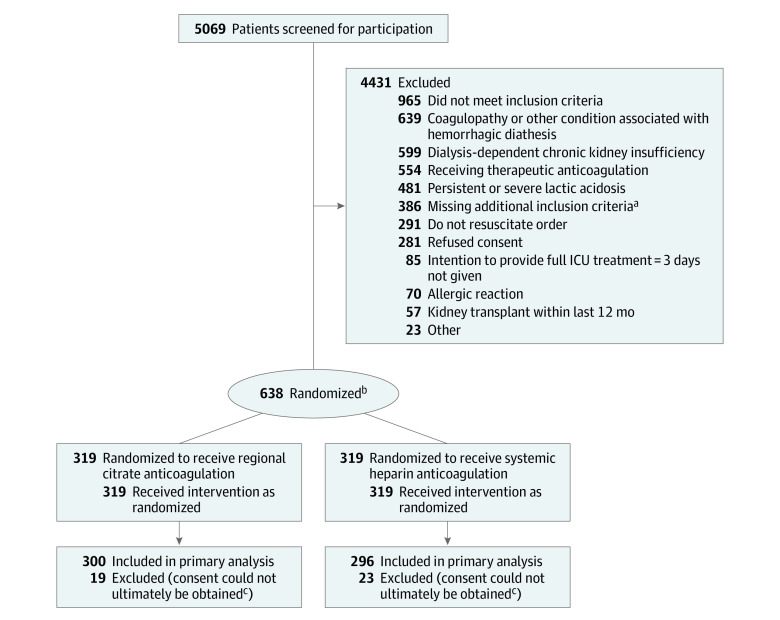
Design, setting, and participants: A parallel-group, randomized multicenter clinical trial in 26 centers across Germany was conducted between March 2016 and December 2018 (final date of follow-up, January 21, 2020). The trial was terminated early after 596 critically ill patients with severe acute kidney injury or clinical indications for initiation of kidney replacement therapy had been enrolled.
Interventions: Patients were randomized to receive either regional citrate anticoagulation (n = 300), which consisted of a target ionized calcium level of 1.0 to 1.40 mg/dL, or systemic heparin anticoagulation (n = 296), which consisted of a target activated partial thromboplastin time of 45 to 60 seconds, for continuous kidney replacement therapy.
Main outcomes and measures: Coprimary outcomes were filter life span and 90-day mortality. Secondary end points included bleeding complications and new infections.
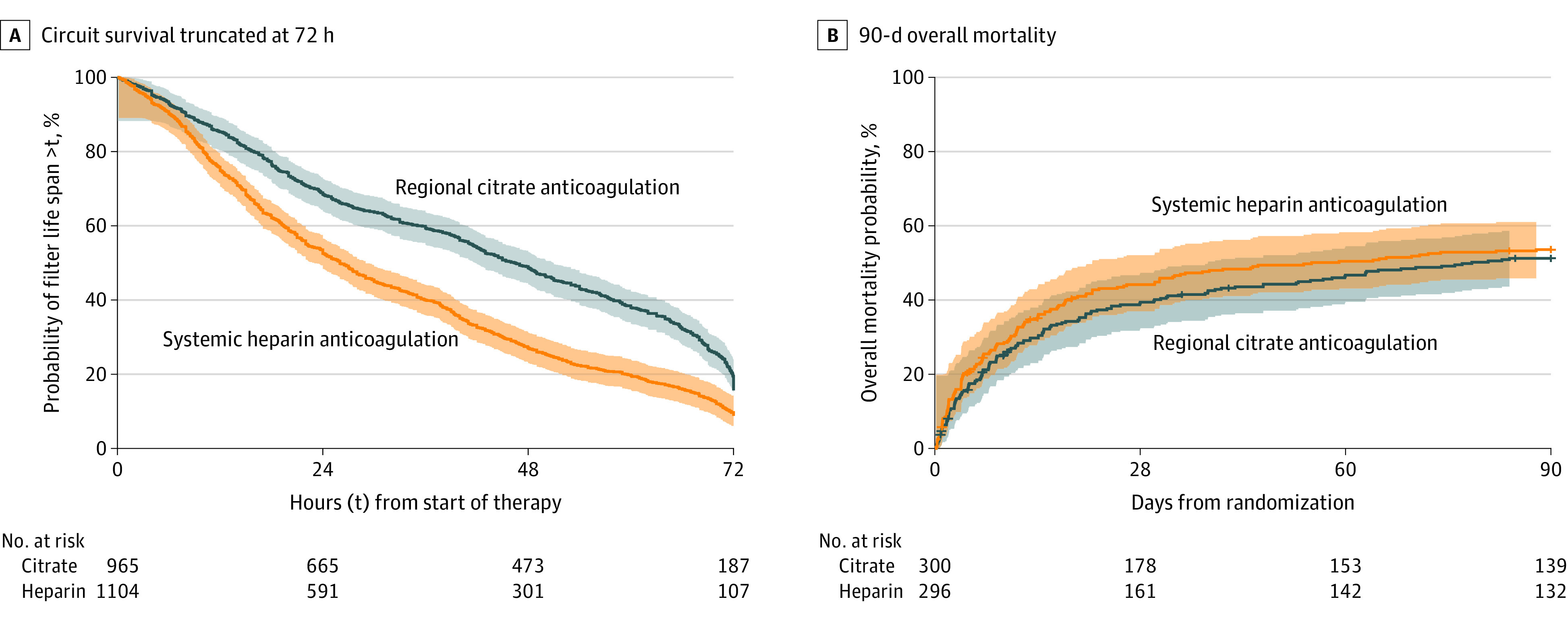
Results: Among 638 patients randomized, 596 (93.4%) (mean age, 67.5 years; 183 [30.7%] women) completed the trial. In the regional citrate group vs systemic heparin group, median filter life span was 47 hours (interquartile range [IQR], 19-70 hours) vs 26 hours (IQR, 12-51 hours) (difference, 15 hours [95% CI, 11 to 20 hours]; P < .001). Ninety-day all-cause mortality occurred in 150 of 300 patients vs 156 of 296 patients (Kaplan-Meier estimator percentages, 51.2% vs 53.6%; unadjusted difference, -2.4% [95% CI, -10.5% to 5.8%]; unadjusted hazard ratio, 0.91 [95% CI, 0.72 to 1.13]; unadjusted P = .38; adjusted difference, -6.1% [95% CI, -12.6% to 0.4%]; primary adjusted hazard ratio, 0.79 [95% CI, 0.63 to 1.004]; primary adjusted P = .054). Of 38 prespecified secondary end points, 34 showed no significant difference. Compared with the systemic heparin group, the regional citrate group had significantly fewer bleeding complications (15/300 [5.1%] vs 49/296 [16.9%]; difference, -11.8% [95% CI, -16.8% to -6.8%]; P < .001) and significantly more new infections (204/300 [68.0%] vs 164/296 [55.4%]; difference, 12.6% [95% CI, 4.9% to 20.3%]; P = .002).
Conclusions and relevance: Among critically ill patients with acute kidney injury receiving continuous kidney replacement therapy, anticoagulation with regional citrate, compared with systemic heparin anticoagulation, resulted in significantly longer filter life span. The trial was terminated early and was therefore underpowered to reach conclusions about the effect of anticoagulation strategy on mortality.
Trial registration: ClinicalTrials.gov Identifier: NCT02669589.
Conflict of interest statement
Figures
Comment in
-
[Focus on nephrology : Intensive medical care studies 2020/2021].Anaesthesist. 2021 Dec;70(12):1053-1058. doi: 10.1007/s00101-021-00980-1. Epub 2021 Oct 22. Anaesthesist. 2021. PMID: 34677635 German. No abstract available.
References
-
- Kellum J A LN, Aspelin P, Barsoum RS, et al. KDIGO clinical practice guideline for acte kidney injury 2012. Kidney Int Suppl. 2012;2(1):1-138. https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-En...
-
- van de Wetering J, Westendorp RG, van der Hoeven JG, Stolk B, Feuth JD, Chang PC. Heparin use in continuous renal replacement procedures: the struggle between filter coagulation and patient hemorrhage. J Am Soc Nephrol. 1996;7(1):145-150. - PubMed
-
- Gattas DJ, Rajbhandari D, Bradford C, Buhr H, Lo S, Bellomo R. A randomized controlled trial of regional citrate versus regional heparin anticoagulation for continuous renal replacement therapy in critically ill adults. Crit Care Med. 2015;43(8):1622-1629. doi: 10.1097/CCM.0000000000001004 - DOI - PubMed
-
- Schilder L, Nurmohamed SA, Bosch FH, et al. ; CASH Study Group . Citrate anticoagulation versus systemic heparinisation in continuous venovenous hemofiltration in critically ill patients with acute kidney injury: a multi-center randomized clinical trial. Crit Care. 2014;18(4):472. doi: 10.1186/s13054-014-0472-6 - DOI - PMC - PubMed
