

Imbalances in circulating angiogenic factors in the pathophysiology of preeclampsia and related disorders
- PMID: 33096092
- PMCID: PMC8884164
- DOI: 10.1016/j.ajog.2020.10.022
Imbalances in circulating angiogenic factors in the pathophysiology of preeclampsia and related disorders
Abstract
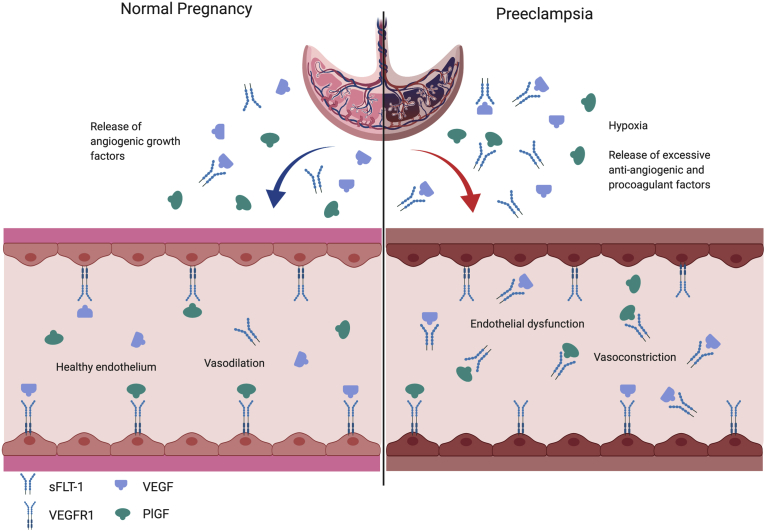
Preeclampsia is a devastating medical complication of pregnancy that can lead to significant maternal and fetal morbidity and mortality. It is currently believed that there is abnormal placentation in as early as the first trimester in women destined to develop preeclampsia. Although the etiology of the abnormal placentation is being debated, numerous epidemiologic and experimental studies suggest that imbalances in circulating angiogenic factors released from the placenta are responsible for the maternal signs and symptoms of preeclampsia. In particular, circulating levels of soluble fms-like tyrosine kinase 1, an antiangiogenic factor, are markedly increased in women with preeclampsia, whereas free levels of its ligand, placental, growth factor are markedly diminished. Alterations in these angiogenic factors precede the onset of clinical signs of preeclampsia and correlate with disease severity. Recently, the availability of automated assays for the measurement of angiogenic biomarkers in the plasma, serum, and urine has helped investigators worldwide to demonstrate a key role for these factors in the clinical diagnosis and prediction of preeclampsia. Numerous studies have reported that circulating angiogenic biomarkers have a very high negative predictive value to rule out clinical disease among women with suspected preeclampsia. These blood-based biomarkers have provided a valuable tool to clinicians to accelerate the time to clinical diagnosis and minimize maternal adverse outcomes in women with preeclampsia. Angiogenic biomarkers have also been useful to elucidate the pathogenesis of related disorders of abnormal placentation such as intrauterine growth restriction, intrauterine fetal death, twin-to-twin transfusion syndrome, and fetal hydrops. In summary, the discovery and characterization of angiogenic proteins of placental origin have provided clinicians a noninvasive blood-based tool to monitor placental function and health and for early detection of disorders of placentation. Uncovering the mechanisms of altered angiogenic factors in preeclampsia and related disorders of placentation may provide insights into novel preventive and therapeutic options.
Keywords: bronchopulmonary dysplasia; cardiovascular disease; fetal death; fetal hydrops; glomerular endotheliosis; hypertension; intrauterine growth restriction; placental-derived growth factor; proteinuria; soluble endoglin; spiral artery remodeling; twin-to-twin transfusion syndrome; vascular endothelial growth factor.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Villar J., Abalos E., Nardin J.M., Merialdi M., Carroli G. Strategies to prevent and treat preeclampsia: evidence from randomized controlled trials. Semin Nephrol. 2004;24:607–615. - PubMed
-
- Wang A., Rana S., Karumanchi S.A. Preeclampsia: the role of angiogenic factors in its pathogenesis. Physiology (Bethesda) 2009;24:147–158. - PubMed
-
- Page E.W. The relation between hydatid moles, relative ischaemia of the gravid uterus and the placental origin of eclampsia. Am J Obstet Gynecol. 1939;37:291–293.
-
- Matsuo K., Kooshesh S., Dinc M., Sun C.C., Kimura T., Baschat A.A. Late postpartum eclampsia: report of two cases managed by uterine curettage and review of the literature. Am J Perinatol. 2007;24:257–266. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
