

Worldwide inertia to the use of cardiorenal protective glucose-lowering drugs (SGLT2i and GLP-1 RA) in high-risk patients with type 2 diabetes
- PMID: 33097060
- PMCID: PMC7585305
- DOI: 10.1186/s12933-020-01154-w
Worldwide inertia to the use of cardiorenal protective glucose-lowering drugs (SGLT2i and GLP-1 RA) in high-risk patients with type 2 diabetes
Abstract
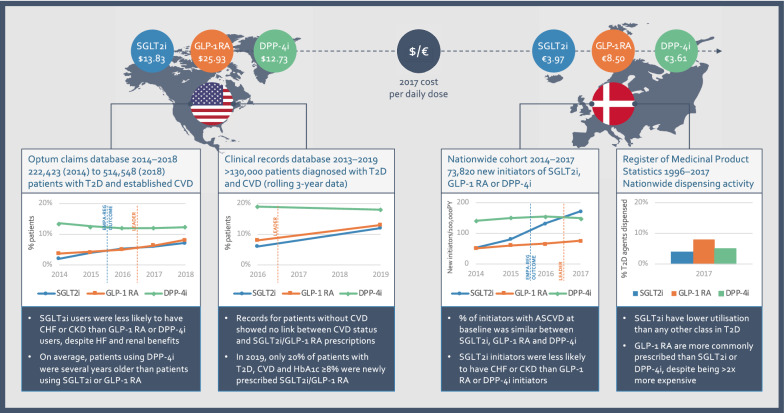
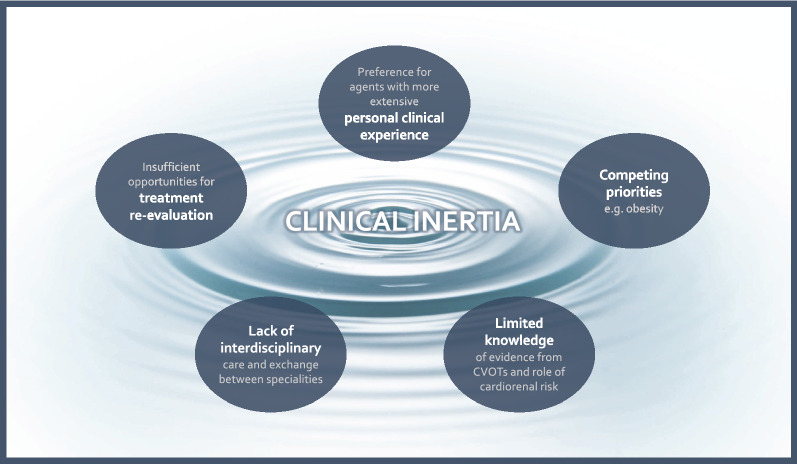
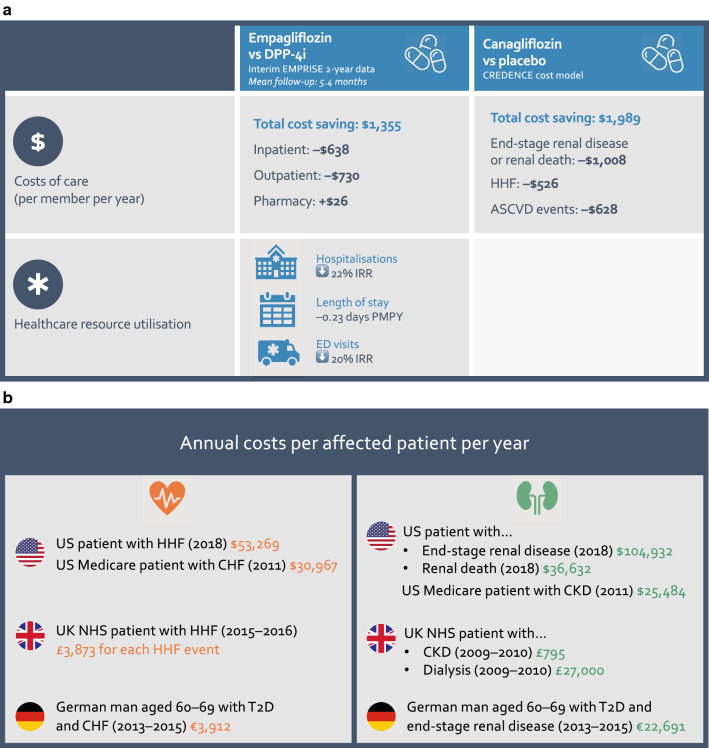
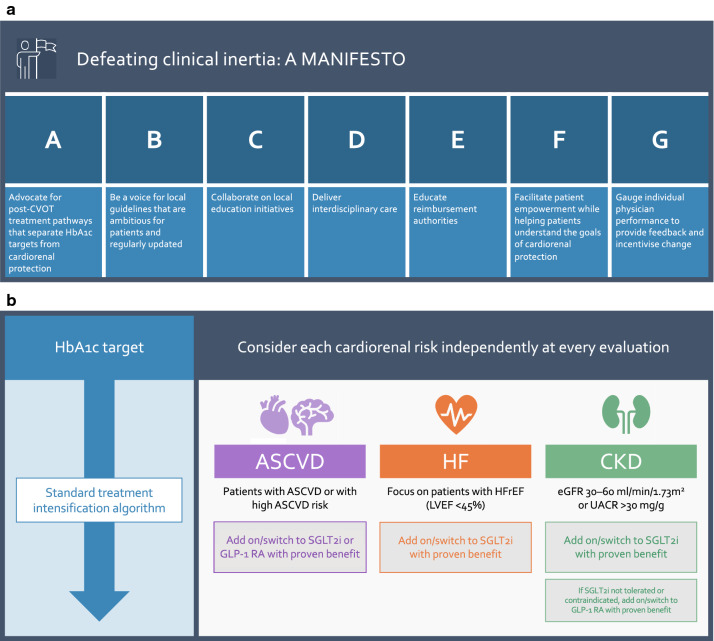
The disclosure of proven cardiorenal benefits with certain antidiabetic agents was supposed to herald a new era in the management of type 2 diabetes (T2D), especially for the many patients with T2D who are at high risk for cardiovascular and renal events. However, as the evidence in favour of various sodium-glucose transporter-2 inhibitor (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RA) accumulates, prescriptions of these agents continue to stagnate, even among eligible, at-risk patients. By contrast, dipeptidyl peptidase-4 inhibitors (DPP-4i) DPP-4i remain more widely used than SGLT2i and GLP-1 RA in these patients, despite a similar cost to SGLT2i and a large body of evidence showing no clear benefit on cardiorenal outcomes. We are a group of diabetologists united by a shared concern that clinical inertia is preventing these patients from receiving life-saving treatments, as well as placing them at greater risk of hospitalisation for heart failure and progression of renal disease. We propose a manifesto for change, in order to increase uptake of SGLT2i and GLP-1 RA in appropriate patients as a matter of urgency, especially those who could be readily switched from an agent without proven cardiorenal benefit. Central to our manifesto is a shift from linear treatment algorithms based on HbA1c target setting to parallel, independent considerations of atherosclerotic cardiovascular disease, heart failure and renal risks, in accordance with newly updated guidelines. Finally, we call upon all colleagues to play their part in implementing our manifesto at a local level, ensuring that patients do not pay a heavy price for continued clinical inertia in T2D.
Keywords: Cardiorenal protection; Clinical inertia; Glucose lowering drugs; Type 2 diabetes.
Conflict of interest statement
GS has received honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Mundipharma, Servier and Takeda for speaking at sponsored meetings or attending advisory boards. NS has participated in scientific advisory boards and/or received honoraria from Astra Zeneca, Novo Nordisk, MSD, Boehringer-Ingelheim, Eli Lilly, Sanofi Aventis. ASA has participated in scientific advisory boards and/or received honoraria from Novo Nordisk, Sanofi-aventis, Boehringer- Ingelheim, Servier, Takeda, Eli Lilly, Astra Zeneca, MSD. AVB has participated in scientific advisory boards and/or received honoraria from Boehringer-Ingelheim, Astra-Zeneca, Novo-Nordisk, Sanofi-Aventis, Eli-Lilly, Novartis, Servier, Janssen, Medtronic. FE has participated in scientific advisory boards and/or received honoraria from Astra Zeneca, Boehringer-Ingelheim, Novo Nordisk. PF has received honoraria as a speaker and participated in scientific advisory-board in the last 3 years for Astra-Zeneca, Janssen, Boehringer Ingelheim, Eli Lilly, Sanofi, Novo Nordisk; has been an investigator of the Empa-Reg Outcome study, the ELIXA trial, the EXSCEL trial and the ongoing SOUL-Study. AJ has served as a consultant and is on speakers bureaus for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme (MSD), Novo Nordisk, and Sanofi. PK has been a board member and/or received honoraria from Novo Nordisk, Sanofi-Aventis, Eli-Lilly, Boehringer-Ingelheim, Astra-Zeneca, Egis, MSD, DiCare, Wörwag-Pharma, Richter-Gedeon, Novartis, 77 Elektronika Kft. IK has been a member of advisory boards and/or received honoraria/speaker fee from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Ipsen, Novo Nordisk, Merck Sharp & Dohme, Sanofi Aventis, Berlin-Chemie. NML has been a member of advisory boards and/or received honoraria /speaker fee from Astra Zeneca, Boehringer-Ingelheim, Eli Lilly, Merck, Novo Nordisk, Sanofi Aventis. BM has been a member of advisory boards and/or received honoraria from Novo Nordisk, Astra Zeneca, Boehringer-Ingelheim, Takeda. EM has been a member of advisory boards and/or received speaker fee from Boehringer-Ingelheim, Eli Lilly, NovoNordisk, Sanofi, MSD, Worwag -Pharma, Mundipharma. DR has been a member of advisory boards and/or received honoraria/speaker fee from Abbott, Amgen, AstraZeneca, Bayer, Belupo, Boehringer Ingelheim, Eli Lilly, Lifescan – Johnson & Johnson, International Sweeteners Association, Krka, Medtronic, Mediligo, Novartis, Novo Nordisk, MSD, Merck Sharp & Dohme, Pfizer, Pliva, Roche, Salvus, Sandoz, Solvay, Sanofi Aventis and Takeda. CS has been a member of advisory boards, received honoraria/fees from Sanofi, Novo Nordisk, Astra Zeneca, Boehringer-Ingellheim, Servier Pharma. JS has been a member of boards and/or received honoraria from Novo Nordisk, Astra Zeneca, Eli Lilly, Sanofi-Aventis, Boehringer-Ingelheim. TT has been a member of advisory board and/or received speaker fee from Boehringer-Ingelheim, Astra Zeneca, Novo Nordisk, Eli Lilly, Sanofi, Servier, MSD. ZV has been a member of advisory boards and/or received honoraria from Astra Zeneca, Novo Nordisk, Boehringer-Ingelheim, Eli Lilly, Sanofi Aventis.
Figures

References
-
- Mosenzon O, Wiviott SD, Cahn A, Rozenberg A, Yanuv I, Goodrich EL, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019;7:606–617. doi: 10.1016/S2213-8587(19)30180-9. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
