

Lung metastases from intraductal papillary neoplasm of the bile duct: a case report
- PMID: 33097064
- PMCID: PMC7585296
- DOI: 10.1186/s12957-020-02054-9
Lung metastases from intraductal papillary neoplasm of the bile duct: a case report
Abstract
Background: Intraductal papillary neoplasm of the bile duct (IPNB) is considered a pre-cancerous biliary lesion and/or an early cancer lesion, although its classification remains unclear. The 2019 revised edition of the World Health Organization Classification of Tumors of the Digestive System proposed type 1 and type 2 as new classification categories, and meta-analyses and/or multi-center cohort studies are beginning to be reported. However, treatment for IPNB recurrence and metastasis remains unclear.
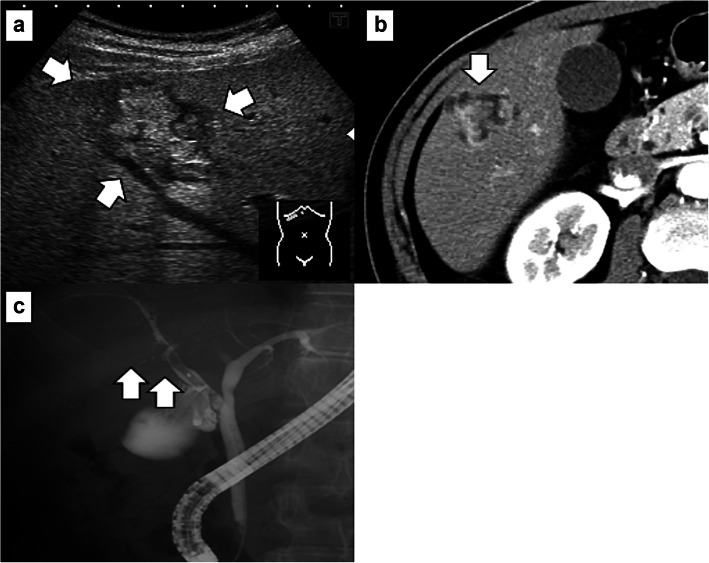
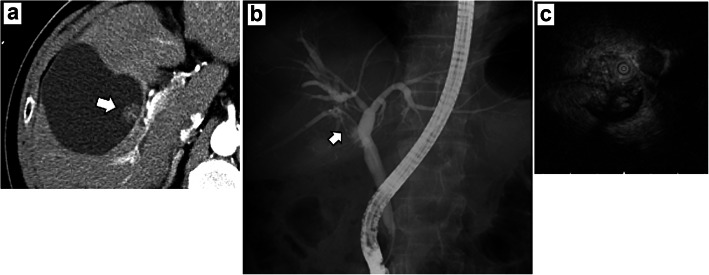
Case presentation: A 60-year-old man who was referred to our hospital after a suspected liver tumor was diagnosed using abdominal ultrasonography. Imaging findings revealed an irregularly shaped tumor in segment 5 (S5) of the liver (size 20 mm). The S5 lesion was suspected as IPNB, and segmentectomy was performed. The pathological findings revealed invasive carcinoma derived from IPNB, and immunohistochemistry revealed positive expression of MUC1, MUC5AC, and MUC6, but negative expression of CDX2 and MUC2. At 9 months after the surgery, computed tomography revealed a tumor in the right bile duct, which was diagnosed as liver recurrence of IPNB, and right hepatectomy was performed. The histopathological findings were the same as for the first resected specimen (i.e., IPNB). At 45 months after the second surgery, computed tomography revealed nodules in both lungs, which were diagnosed as lung metastases from IPNB and resected in two separate procedures. The pathological findings were metastatic carcinoma from IPNB for both lung lesions. The patient is currently alive and undergoing adjuvant chemotherapy (S-1), which was initiated 64 months after the first resection and 12 months after resection of the lung metastases.
Conclusion: We encountered a rare case of lung metastases from IPNB, which were diagnosed immunohistologically. Because IPNB is generally a slow-growing tumor, resection may be feasible for IPNB recurrence and/or metastasis, which may be detected during long-term follow-up. Thus, even if resection is performed for primary IPNB, additional surgical treatment may be feasible in this setting.
Keywords: IPNB; Intraductal papillary neoplasm of the bile duct; Lung metastasis; Re-resection; Recurrence; Surgery.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Nakamura Y, Bastruk O, Esposito I, Klimstra DS, Komuta M, Zen Y. Intraductal papillary neoplasm of the bile duct. In: WHO Classification of Tumors Editorial Board. Digestive System Tumors WHO Classification of Tumors. 5th ed: World Health Organization; 2019. p. 279–82.
-
- Nakanuma Y, Jang KT, Fukushima N, Furukawa T, Hong SM, Kim H, et al. A statement by the Japan-Korea expert pathologists for future clinicopathological and molecular analyses toward consensus building of intraductal papillary neoplasm of the bile duct through several opinions at the present stage. J Hepatobiliary Pancreat Sci. 2018;25:181–187. doi: 10.1002/jhbp.532. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
