

Dementia in late-onset epilepsy: The Atherosclerosis Risk in Communities study
- PMID: 33097597
- PMCID: PMC7836657
- DOI: 10.1212/WNL.0000000000011080
Dementia in late-onset epilepsy: The Atherosclerosis Risk in Communities study
Abstract
Objective: To determine the risk of dementia after the development of late-onset epilepsy.
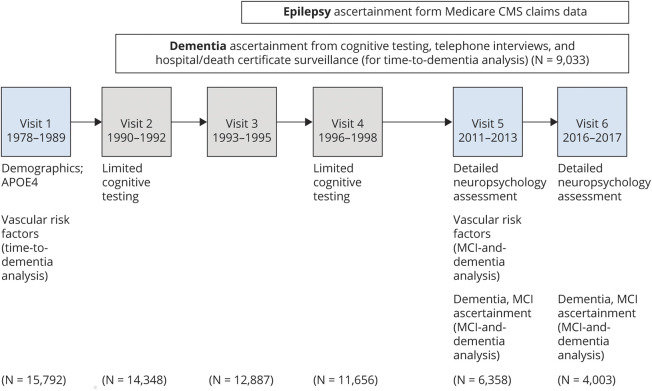
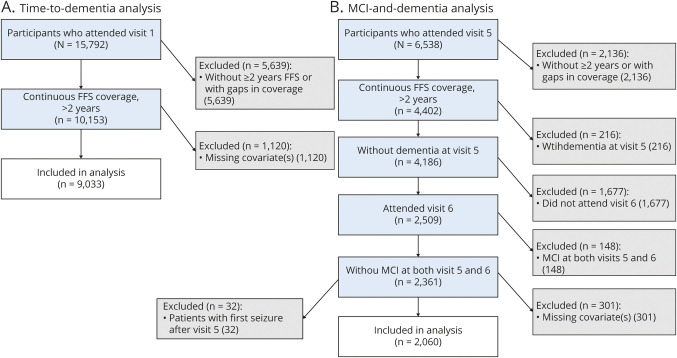
Methods: We used data from the Atherosclerosis Risk in Communities (ARIC) cohort study, which started in 1987 to 1989 with 15,792 mostly Black and White men and women from 4 US communities. We identified late-onset epilepsy (LOE; seizures starting at age 67 or later) from linked Medicare claims data. We used a Cox proportional hazards regression model to evaluate associations between LOE and dementia through 2017 as ascertained from neuropsychological testing, interviews, and hospital discharge surveillance, and we used multinomial logistic regression to assess the risk of dementia and mild cognitive impairment in the subset with full neuropsychological assessments available. We adjusted for demographics and vascular and Alzheimer disease risk factors.
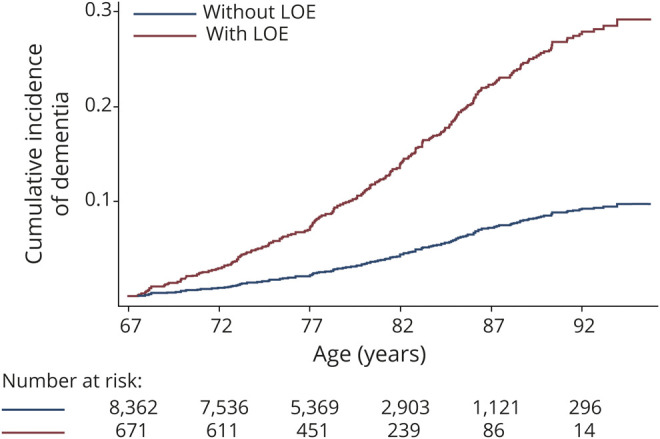
Results: Of 9,033 ARIC participants with sufficient Medicare coverage data (4,980 [55.1%] female, 1993 [22.1%] Black), 671 met the definition of LOE. Two hundred seventy-nine (41.6%) participants with and 1,408 (16.8%) without LOE developed dementia (p < 0.001). After a diagnosis of LOE, the adjusted hazard ratio for developing subsequent dementia was 3.05 (95% confidence interval 2.65-3.51). The median time to dementia ascertainment after the onset of LOE was 3.66 years (quartile 1-3, 1.28-8.28 years).
Interpretation: The risk of incident dementia is substantially elevated in individuals with LOE. Further work is needed to explore causes for the increased risk of dementia in this growing population.
© 2020 American Academy of Neurology.
Figures
Comment in
-
Dementia and epilepsy: Not a one-way street.Neurology. 2020 Dec 15;95(24):1074-1075. doi: 10.1212/WNL.0000000000011084. Epub 2020 Oct 23. Neurology. 2020. PMID: 33097601 No abstract available.
References
-
- Ramsay RE, Rowan AJ, Pryor FM. Special considerations in treating the elderly patient with epilepsy. Neurology 2004;62(suppl 2):S24–S29. - PubMed
-
- Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39–S48. - PubMed
-
- Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935-1984. Epilepsia 1993;34:453–468. - PubMed
-
- Hesdorffer DC, Hauser WA, Annegers JF, Kokmen E, Rocca WA. Dementia and adult-onset unprovoked seizures. Neurology 1996;46:727–730. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous