

Urinary podocyte mRNAs precede microalbuminuria as a progression risk marker in human type 2 diabetic nephropathy
- PMID: 33097787
- PMCID: PMC7584595
- DOI: 10.1038/s41598-020-75320-1
Urinary podocyte mRNAs precede microalbuminuria as a progression risk marker in human type 2 diabetic nephropathy
Abstract
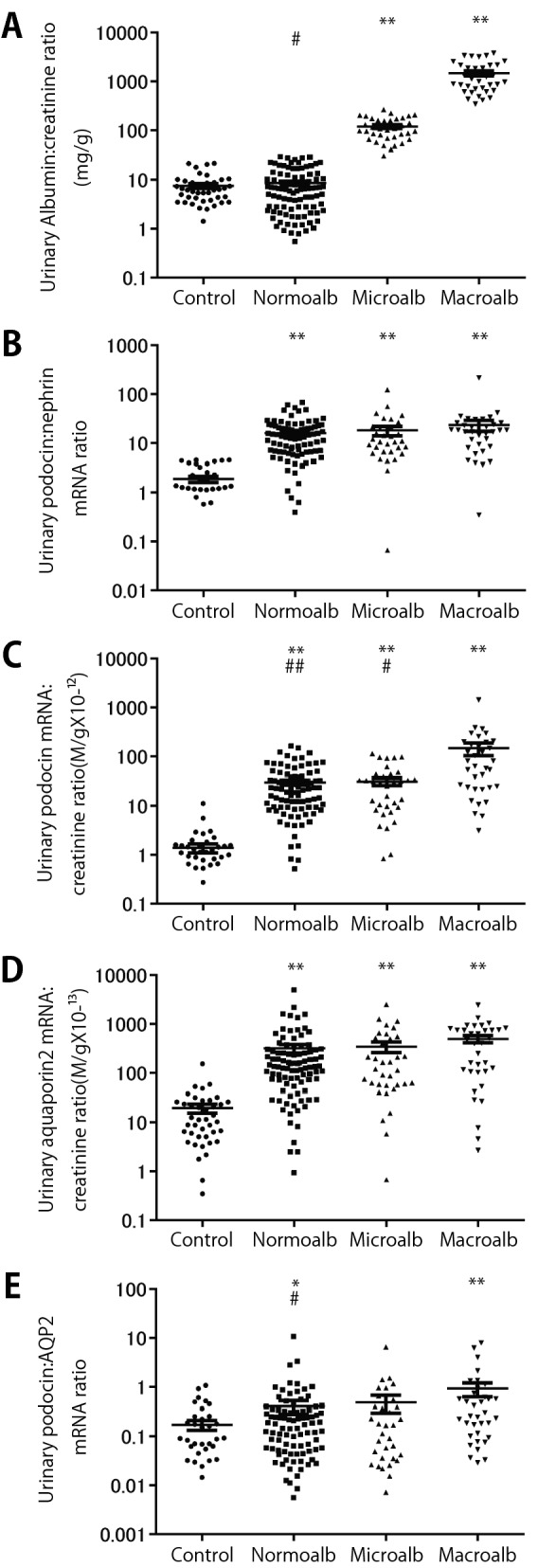
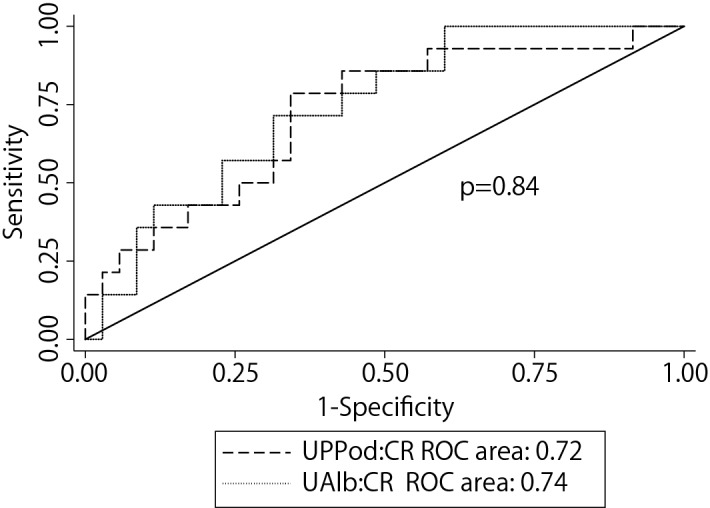
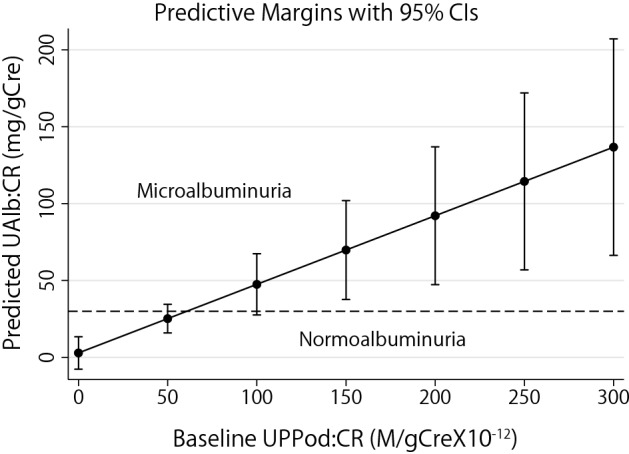
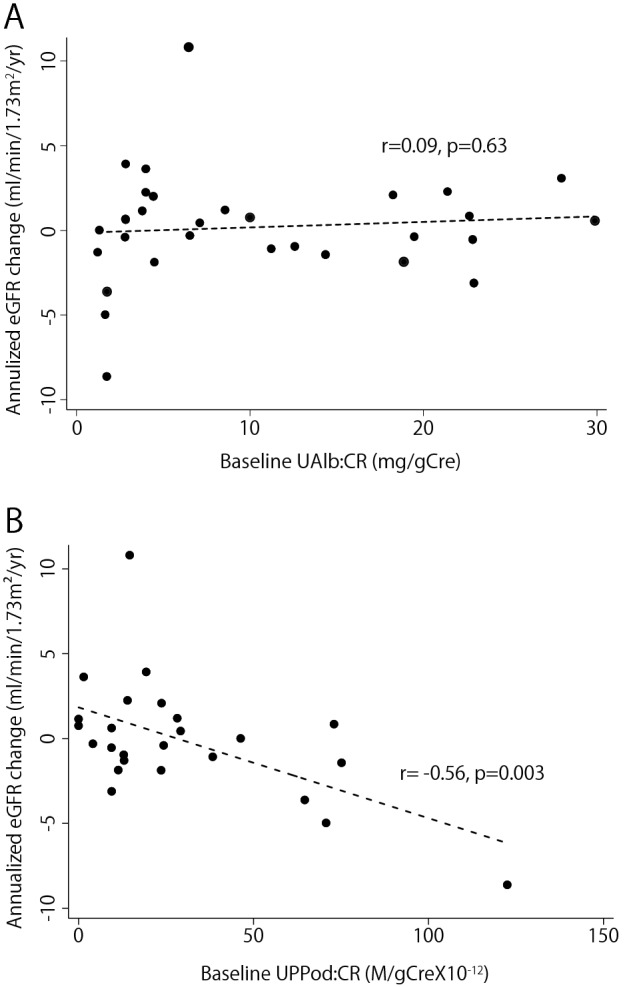
Earlier detection of progression risk in diabetic nephropathy will allow earlier intervention to reduce progression. The hypothesis that urinary pellet podocyte mRNA is a more sensitive progression risk marker than microalbuminuria was tested. A cross sectional cohort of 165 type 2 diabetics and 41 age and sex-matched controls were enrolled. Podocyte stress (Urinary pellet podocin:nephrin mRNA ratio), podocyte detachment (Urinary pellet podocin mRNA:creatinine ratio: UPPod:CR) and a tubular marker (Urinary pellet aquaporin 2:creatinine ratio) were measured in macro-albuminuric, micro-albuminuric and norm-albuminuric groups. eGFR was reassessed after 4 years in 124 available diabetic subjects. Urinary pellet podocyte and tubular mRNA markers were increased in all diabetic groups in cross-sectional analysis. After 4 years of follow-up univariable and multivariate model analysis showed that the only urinary markers significantly related to eGFR slope were UPPod:CR (P < 0.01) and albuminuria (P < 0.01). AUC analysis using K-fold cross validation to predict eGFR loss of ≥ 3 ml/min/1.73m2/year showed that UPPod:CR and albuminuria each improved the AUC similarly such that combined with clinical variables they gave an AUC = 0.70. Podocyte markers and albuminuria had overlapping AUC contributions, as expected if podocyte depletion causes albuminuria. In the norm-albuminuria cohort (n = 75) baseline UPPod:CR was associated with development of albuminuria (P = 0.007) and, in the tertile with both normal kidney function (eGFR 84 ± 11.7 ml/min/1.73m2) and norm-albuminuria at baseline, UPPod:CR was associated with eGFR loss rate (P = 0.003). In type 2 diabetics with micro- or macro-albuminuria UPPod:CR and albuminuria were equally good at predicting eGFR loss. For norm-albuminuric type 2 diabetics UPPod:CR predicted both albuminuria and eGFR loss.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
