

Adipocyte lipolysis drives acute stress-induced insulin resistance
- PMID: 33097799
- PMCID: PMC7584576
- DOI: 10.1038/s41598-020-75321-0
Adipocyte lipolysis drives acute stress-induced insulin resistance
Abstract
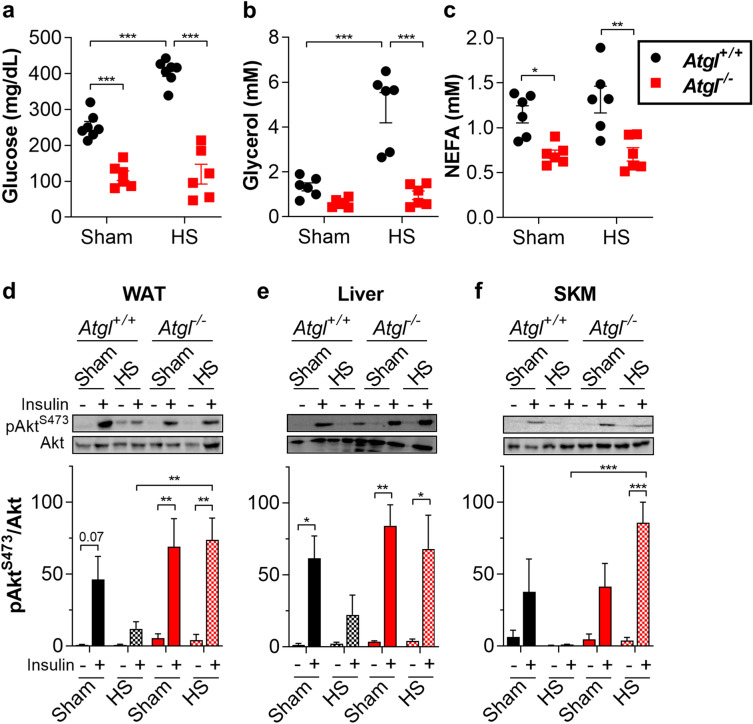
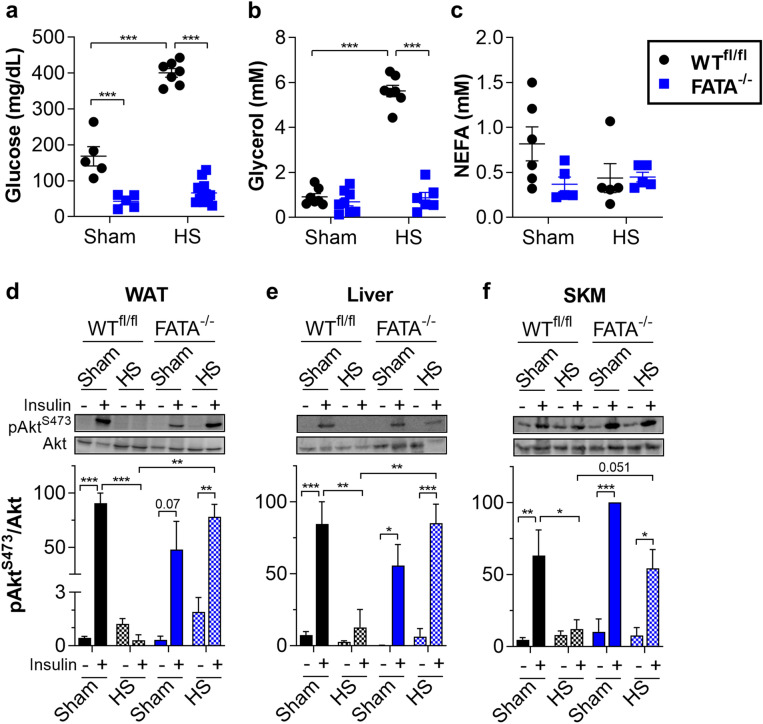
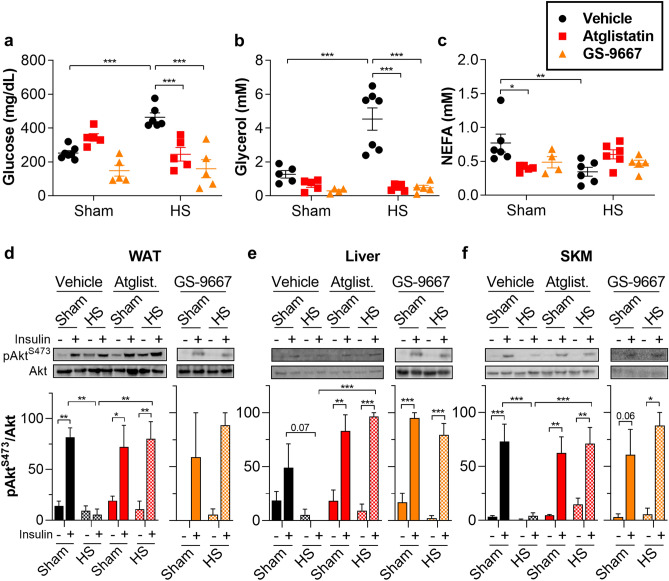
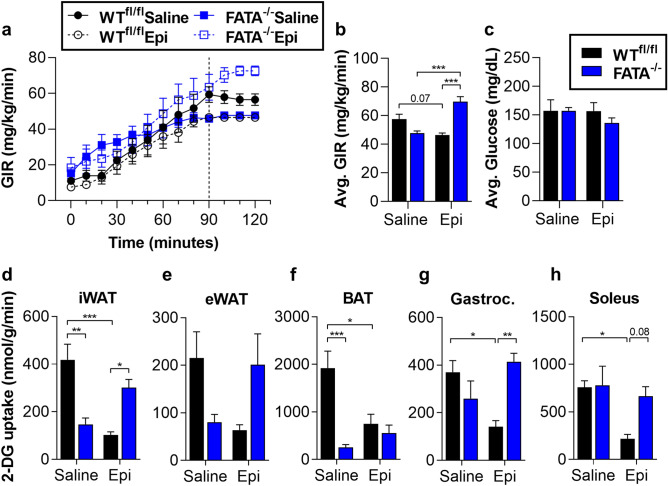
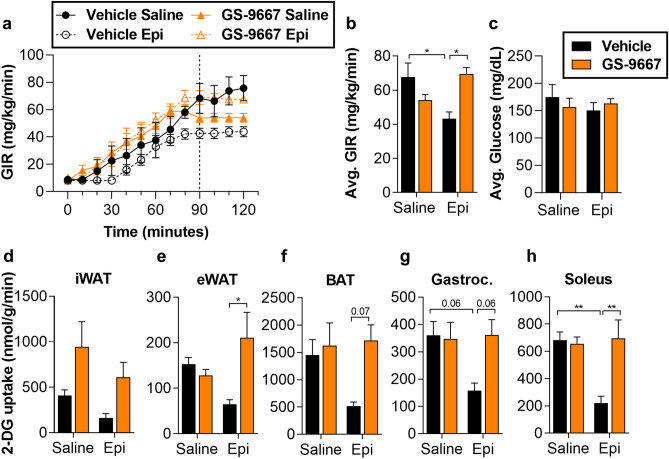
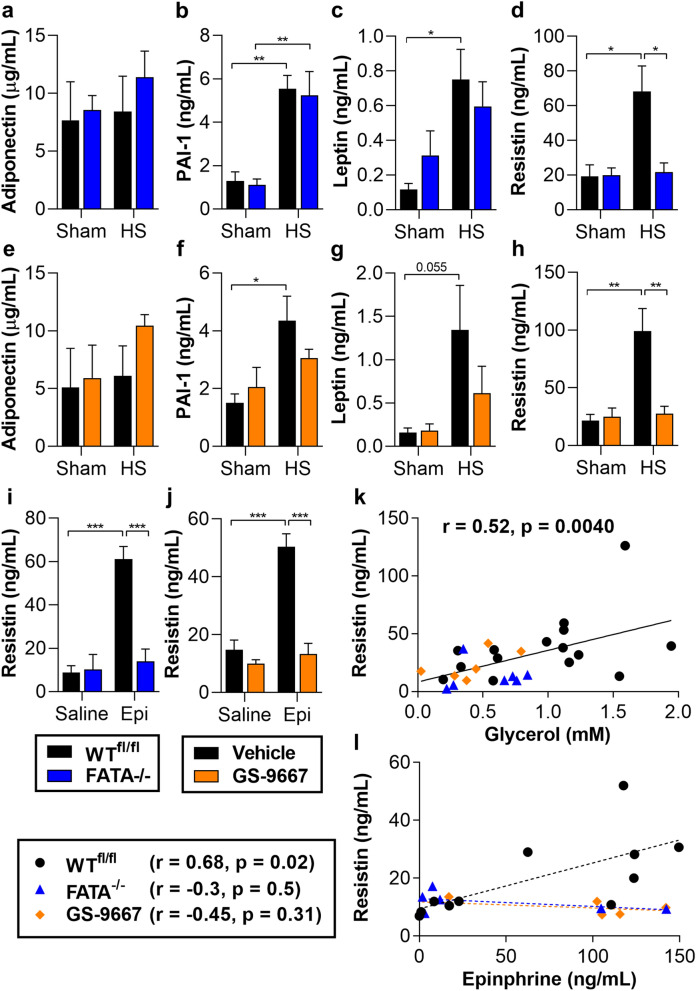
Stress hyperglycemia and insulin resistance are evolutionarily conserved metabolic adaptations to severe injury including major trauma, burns, or hemorrhagic shock (HS). In response to injury, the neuroendocrine system increases secretion of counterregulatory hormones that promote rapid mobilization of nutrient stores, impair insulin action, and ultimately cause hyperglycemia, a condition known to impair recovery from injury in the clinical setting. We investigated the contributions of adipocyte lipolysis to the metabolic response to acute stress. Both surgical injury with HS and counterregulatory hormone (epinephrine) infusion profoundly stimulated adipocyte lipolysis and simultaneously triggered insulin resistance and hyperglycemia. When lipolysis was inhibited, the stress-induced insulin resistance and hyperglycemia were largely abolished demonstrating an essential requirement for adipocyte lipolysis in promoting stress-induced insulin resistance. Interestingly, circulating non-esterified fatty acid levels did not increase with lipolysis or correlate with insulin resistance during acute stress. Instead, we show that impaired insulin sensitivity correlated with circulating levels of the adipokine resistin in a lipolysis-dependent manner. Our findings demonstrate the central importance of adipocyte lipolysis in the metabolic response to injury. This insight suggests new approaches to prevent insulin resistance and stress hyperglycemia in trauma and surgery patients and thereby improve outcomes.
Conflict of interest statement
V.R., A.K., and T.E.H. are inventors on a patent application relevant to this study filed by the University of Virginia through the UVA Licensing & Ventures Group (15/760,990). No other authors declare competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
