

Longitudinal analysis of surgical outcome in subjects with pulsatile tinnitus originating from the sigmoid sinus
- PMID: 33097817
- PMCID: PMC7584625
- DOI: 10.1038/s41598-020-75348-3
Longitudinal analysis of surgical outcome in subjects with pulsatile tinnitus originating from the sigmoid sinus
Abstract
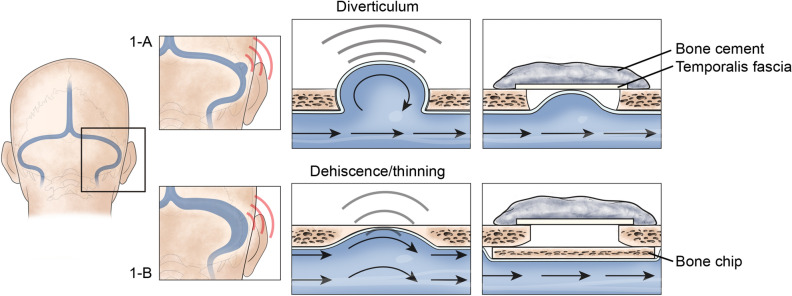
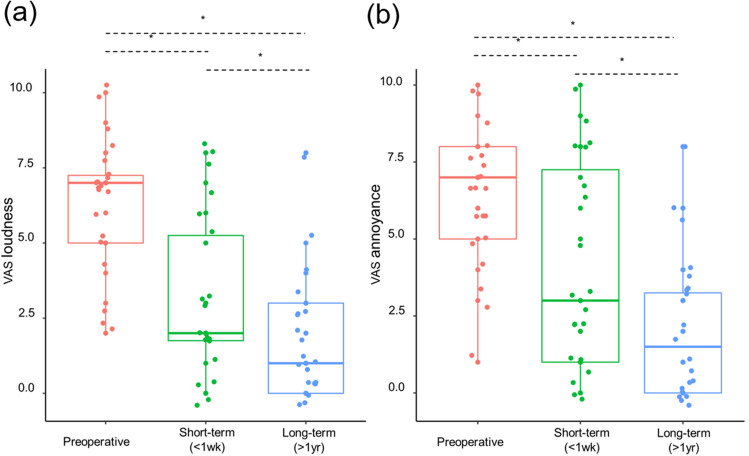
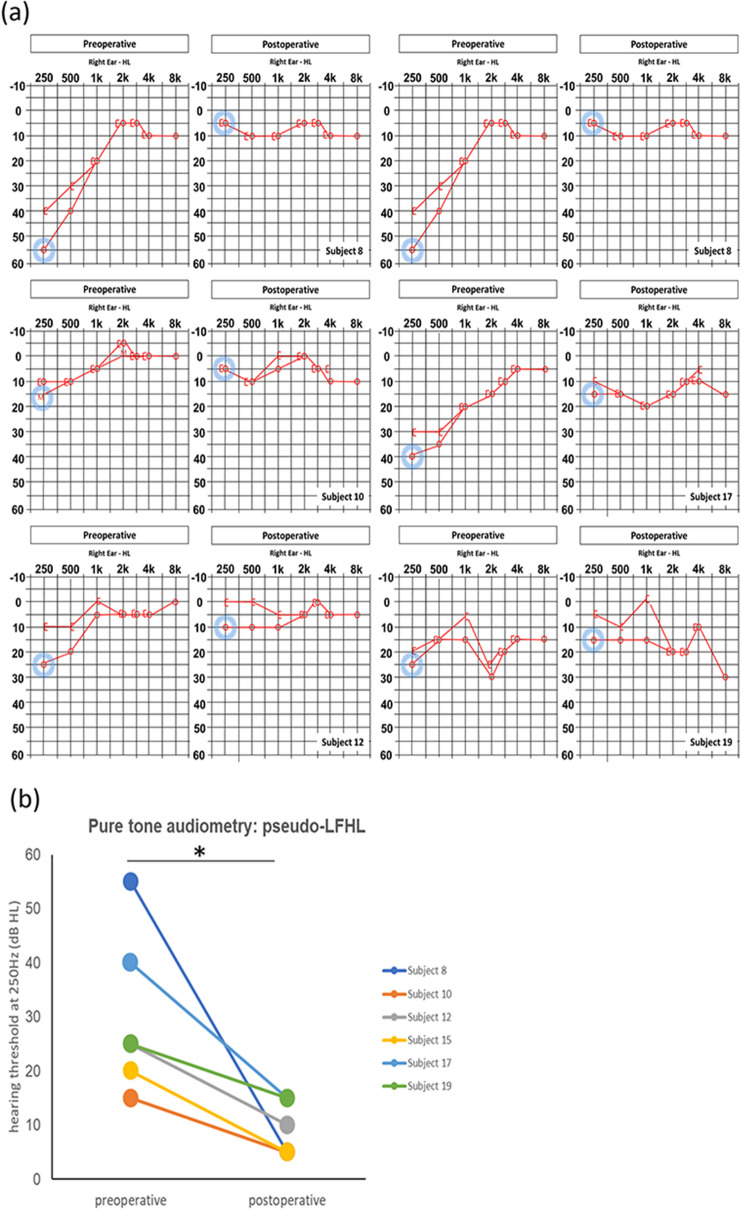
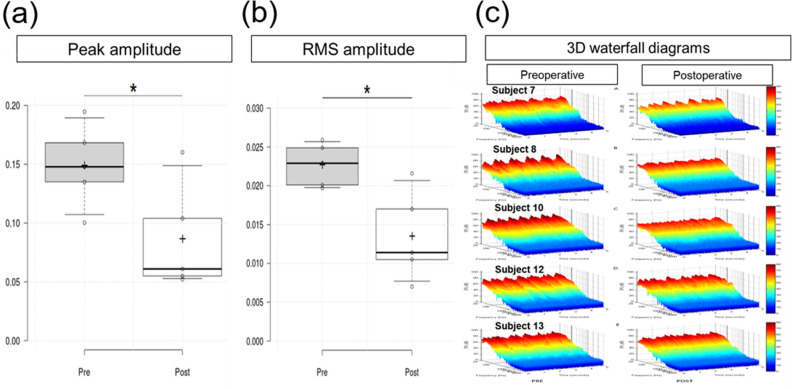
A dominant sigmoid sinus with either diverticulum or dehiscence (SS-Div/SS-Deh) is a common cause of pulsatile tinnitus (PT). For PT originating from SS-Div/SS-Deh, an etiology-specific and secure reconstruction using firm materials is vital for optimal outcomes. As a follow-up to our previous reports on transmastoid SS resurfacing or reshaping for SS-Div/SS-Deh, this study aimed to evaluate the long-term results of transmastoid resurfacing/reshaping. We retrospectively reviewed 20 PT patients who were diagnosed with SS-Div/SS-Deh, underwent transmastoid resurfacing/reshaping, and were followed up for more than 1 year postoperatively. For PT, immediate and long-term changes (> 1 year) in loudness and annoyance were analyzed using the visual analog scale (VAS). Additionally, pre and postoperative objective measurements of PT using transcanal sound recording and spectro-temporal analysis (TSR-STA), imaging results, and audiological findings were comprehensively analyzed. Significant improvements in PT were sustained or enhanced for > 1 year (median follow-up period: 37 months, range: 12-54 months). On TSR-STA, both peak and root mean square amplitudes decreased after surgery. Also, the average pure-tone threshold at 250 Hz improved after surgery. Thus, our long-term follow-up data confirmed that the surgical management of PT originating from SS-Div/SS-Deh is successful with regard to both objective and subjective measures.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Transmastoid reshaping of the sigmoid sinus: preliminary study of a novel surgical method to quiet pulsatile tinnitus of an unrecognized vascular origin.J Neurosurg. 2016 Aug;125(2):441-9. doi: 10.3171/2015.6.JNS15961. Epub 2016 Jan 8. J Neurosurg. 2016. PMID: 26745481
-
Sinus Wall Resurfacing for Patients With Temporal Bone Venous Sinus Diverticulum and Ipsilateral Pulsatile Tinnitus.Neurosurgery. 2015 Nov;77(5):709-17; discussion 717. doi: 10.1227/NEU.0000000000000902. Neurosurgery. 2015. PMID: 26197352
-
Transmastoid Hydroxyapatite Resurfacing for Sigmoid Sinus Wall Anomalies Causing Pulsatile Tinnitus.Ann Otol Rhinol Laryngol. 2021 Aug;130(8):885-891. doi: 10.1177/0003489420987407. Epub 2021 Jan 8. Ann Otol Rhinol Laryngol. 2021. PMID: 33412915
-
Surgical management of pulsatile tinnitus secondary to jugular bulb or sigmoid sinus diverticulum with review of literature.Am J Otolaryngol. 2018 Mar-Apr;39(2):247-252. doi: 10.1016/j.amjoto.2017.12.019. Epub 2017 Dec 29. Am J Otolaryngol. 2018. PMID: 29336902 Review.
-
Systematic Review of Temporal Bone-Resurfacing Techniques for Pulsatile Tinnitus Associated with Vascular Wall Anomalies.Otolaryngol Head Neck Surg. 2019 May;160(5):749-761. doi: 10.1177/0194599818823205. Epub 2019 Jan 22. Otolaryngol Head Neck Surg. 2019. PMID: 30667295
Cited by
-
Therapeutic Validation of Venous Pulsatile Tinnitus and Biomaterial Applications for Temporal Bone Reconstruction Surgery Using Multi-sensing Platforms and Coupled Computational Techniques.Front Bioeng Biotechnol. 2022 Jan 3;9:777648. doi: 10.3389/fbioe.2021.777648. eCollection 2021. Front Bioeng Biotechnol. 2022. PMID: 35047487 Free PMC article.
-
Evidence of air-conduction transmission pathway and strategized transtemporal operative techniques for venous pulsatile tinnitus: Combining water occlusion test and operative sensing applications.Laryngoscope Investig Otolaryngol. 2021 Nov 15;6(6):1436-1448. doi: 10.1002/lio2.699. eCollection 2021 Dec. Laryngoscope Investig Otolaryngol. 2021. PMID: 34938885 Free PMC article.
-
The Effect of Degree of Temporal Bone Pneumatization on Sound Transmission of Pulsatile Tinnitus Induced by Sigmoid Sinus Diverticulum and/or Dehiscence: A Clinical and Experimental Study.J Int Adv Otol. 2021 Jul;17(4):319-324. doi: 10.5152/iao.2021.9449. J Int Adv Otol. 2021. PMID: 34309552 Free PMC article.
-
Preoperative Significance of Ipsilateral Manual Neck Compression in Patients With Pulsatile Tinnitus Secondary to Sigmoid Sinus Dehiscences and Diverticula.Front Neurol. 2022 Mar 17;13:869244. doi: 10.3389/fneur.2022.869244. eCollection 2022. Front Neurol. 2022. PMID: 35370915 Free PMC article.
-
Causes and outcomes of revision surgery in subjects with pulsatile tinnitus.Front Neurol. 2023 Jul 24;14:1215636. doi: 10.3389/fneur.2023.1215636. eCollection 2023. Front Neurol. 2023. PMID: 37554389 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
