

Impact of Bridging Locoregional Therapies for Hepatocellular Carcinoma on Post-transplant Clinical Outcome
- PMID: 33098134
- PMCID: PMC10367045
- DOI: 10.1111/ctr.14128
Impact of Bridging Locoregional Therapies for Hepatocellular Carcinoma on Post-transplant Clinical Outcome
Abstract
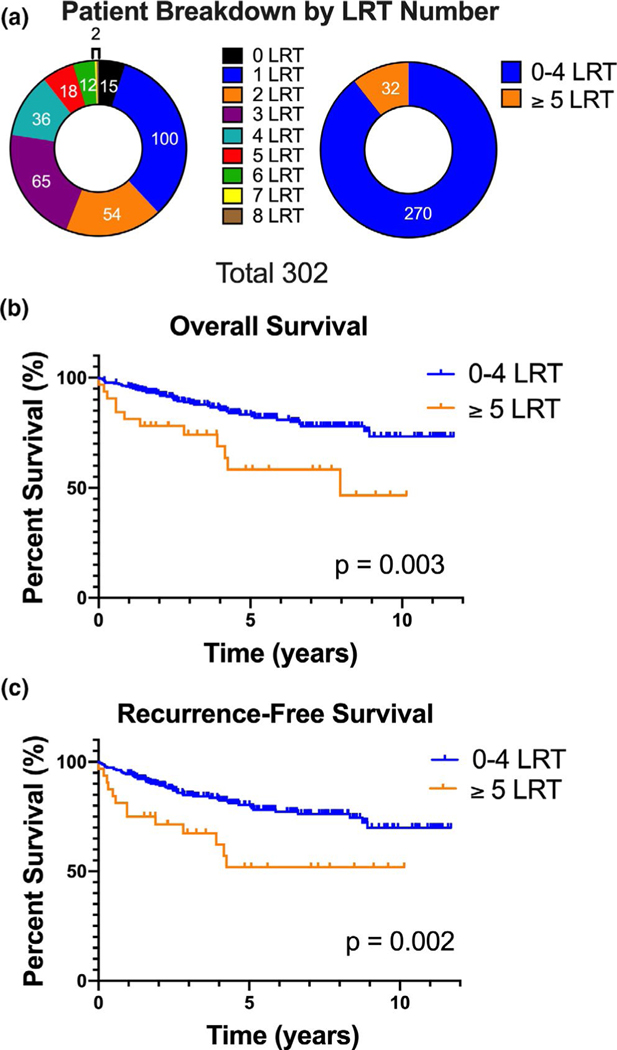
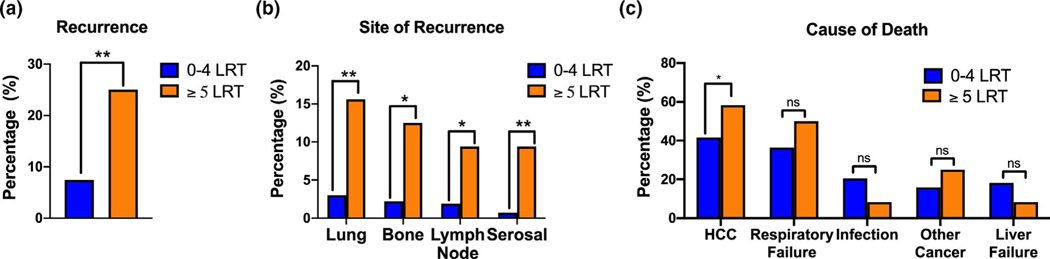
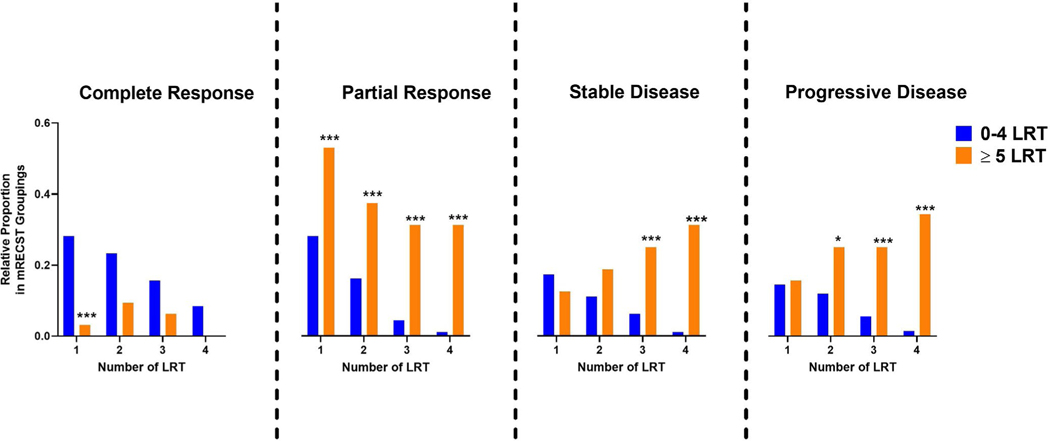
Long waiting times due to ongoing organ shortage have led to increased utilization of locoregional therapies (LRTs) to bridge patients with hepatocellular carcinoma (HCC) to liver transplantation (LT). We performed this study to evaluate the impact of LRTs on post-LT outcomes. We conducted a retrospective study of patients who were transplanted for HCC at Stanford University Hospital between 2008 and 2018 (n = 302). We found that receipt of ≥5 LRTs was an independent and significant predictor of poor overall 5-year survival (58.3% vs. 83.3%; HR 2.26, p = .03), poor recurrence-free 5-year survival (51.9% vs. 80.4%; HR 2.12, p = .03), and was associated with higher rates of recurrence (25.0% vs. 7.4%, p = .001). Moreover, recurrent HCC was more likely to be the cause of death (58.3% vs. 41.7%, p = .04) in patients who received ≥5 LRTs. Also, patients who required ≥5 LRTs showed an overall lower rate of radiological complete response (46.9% vs. 97.8%, p = .001) and were more likely to have more advanced pathological stage tumors in the explant (65.6% vs. 29.6%, p < .001). In conclusion, receipt of ≥5 bridging LRTs prior to LT is associated with worse post-transplant clinical outcomes.
Keywords: Hepatocellular carcinoma; Liver cancer; Locoregional therapy; Transarterial chemoembolization; Transplant.
© 2020 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
CONFLICT OF INTEREST
Authors declare no conflicts of interests.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Liu Z, Suo C, Mao X, et al. Global incidence trends in primary liver cancer by age at diagnosis, sex, region, and etiology, 1990–2017. Cancer. 2020;126(10):2267–2278. - PubMed
-
- Hogen R, Lo M, DiNorcia J, et al. More than just wait time? Regional differences in liver transplant outcomes for hepatocellular carcinoma. Transplantation. 2019;103:747–754. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
