

Atrial nitroso-redox balance and refractoriness following on-pump cardiac surgery: a randomized trial of atorvastatin
- PMID: 33098411
- PMCID: PMC8752359
- DOI: 10.1093/cvr/cvaa302
Atrial nitroso-redox balance and refractoriness following on-pump cardiac surgery: a randomized trial of atorvastatin
Abstract
Aims: Systemic inflammation and increased activity of atrial NOX2-containing NADPH oxidases have been associated with the new onset of atrial fibrillation (AF) after cardiac surgery. In addition to lowering LDL-cholesterol, statins exert rapid anti-inflammatory and antioxidant effects, the clinical significance of which remains controversial.
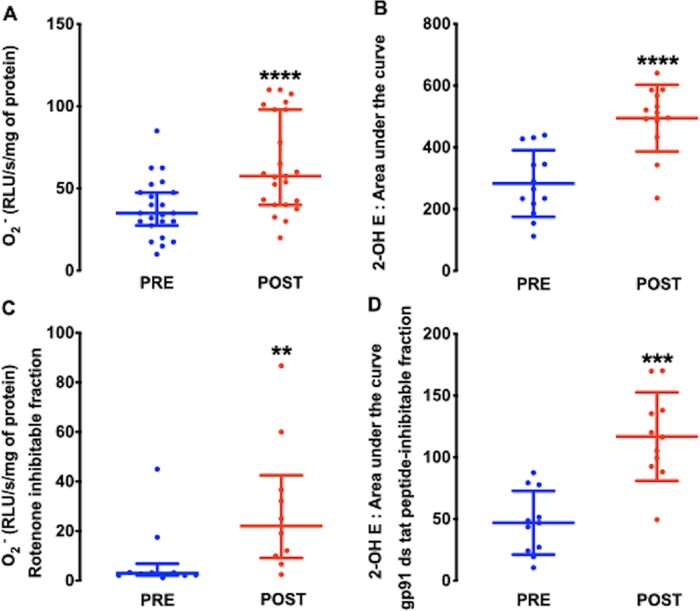
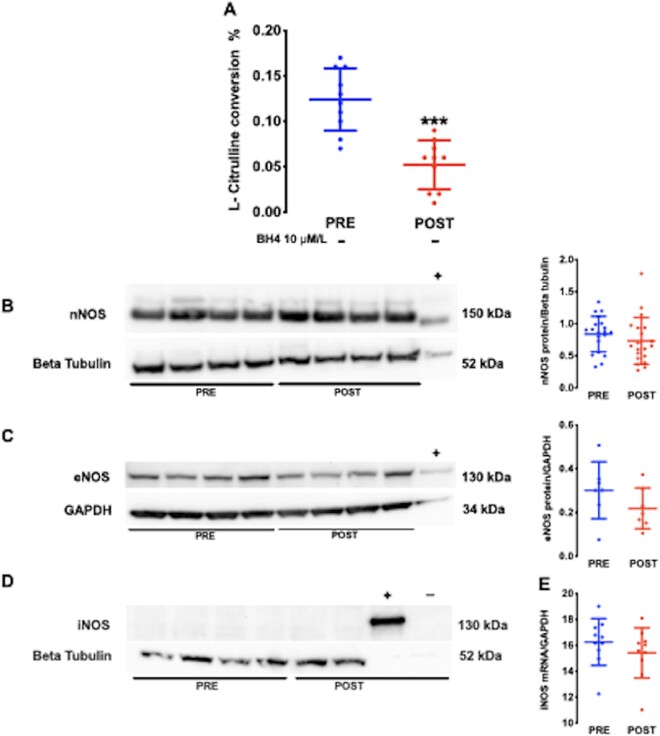
Methods and results: We first assessed the impact of cardiac surgery and cardiopulmonary bypass (CPB) on atrial nitroso-redox balance by measuring NO synthase (NOS) and GTP cyclohydrolase-1 (GCH-1) activity, biopterin content, and superoxide production in paired samples of the right atrial appendage obtained before (PRE) and after CPB and reperfusion (POST) in 116 patients. The effect of perioperative treatment with atorvastatin (80 mg once daily) on these parameters, blood biomarkers, and the post-operative atrial effective refractory period (AERP) was then evaluated in a randomized, double-blind, placebo-controlled study in 80 patients undergoing cardiac surgery on CPB. CPB and reperfusion led to a significant increase in atrial superoxide production (74% CI 71-76%, n = 46 paired samples, P < 0.0001) and a reduction in atrial tetrahydrobiopterin (BH4) (34% CI 33-35%, n = 36 paired samples, P < 0.01), and in GCH-1 (56% CI 55-58%, n = 26 paired samples, P < 0.001) and NOS activity (58% CI 52-67%, n = 20 paired samples, P < 0.001). Perioperative atorvastatin treatment prevented the effect of CPB and reperfusion on all parameters but had no significant effect on the postoperative right AERP, troponin release, or NT-proBNP after cardiac surgery.
Conclusion: Perioperative statin therapy prevents post-reperfusion atrial nitroso-redox imbalance in patients undergoing on-pump cardiac surgery but has no significant impact on postoperative atrial refractoriness, perioperative myocardial injury, or markers of postoperative LV function.
Clinical trial registration: https://clinicaltrials.gov/ct2/show/NCT01780740.
Keywords: Atorvastatin; Atrial refractory period; Clinical trial; Ischaemia-Reperfusion Injury; Nitric Oxide Synthase; Oxidant stress; Postoperative Atrial fibrillation.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures






References
-
- Kim YM, Kattach H, Ratnatunga C, Pillai R, Channon KM, Casadei B. Association of atrial nicotinamide adenine dinucleotide phosphate oxidase activity with the development of atrial fibrillation after cardiac surgery. J Am Coll Cardiol 2008;51:68–74. - PubMed
-
- Levitsky S. Protecting the myocardial cell during coronary revascularization. The William W. L. Glenn Lecture. Circulation 2006;114:I339–I343. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
