

Improving Utilization of Aspirin for Prevention of Preeclampsia in a High-Risk Urban Cohort: A Prospective Cohort Study
- PMID: 33099285
- PMCID: PMC8491097
- DOI: 10.1055/s-0040-1718580
Improving Utilization of Aspirin for Prevention of Preeclampsia in a High-Risk Urban Cohort: A Prospective Cohort Study
Abstract
Objective: This study aimed to evaluate the utilization of aspirin for preeclampsia prevention before and after implementation of a screening tool during nuchal translucency (NT) ultrasound.
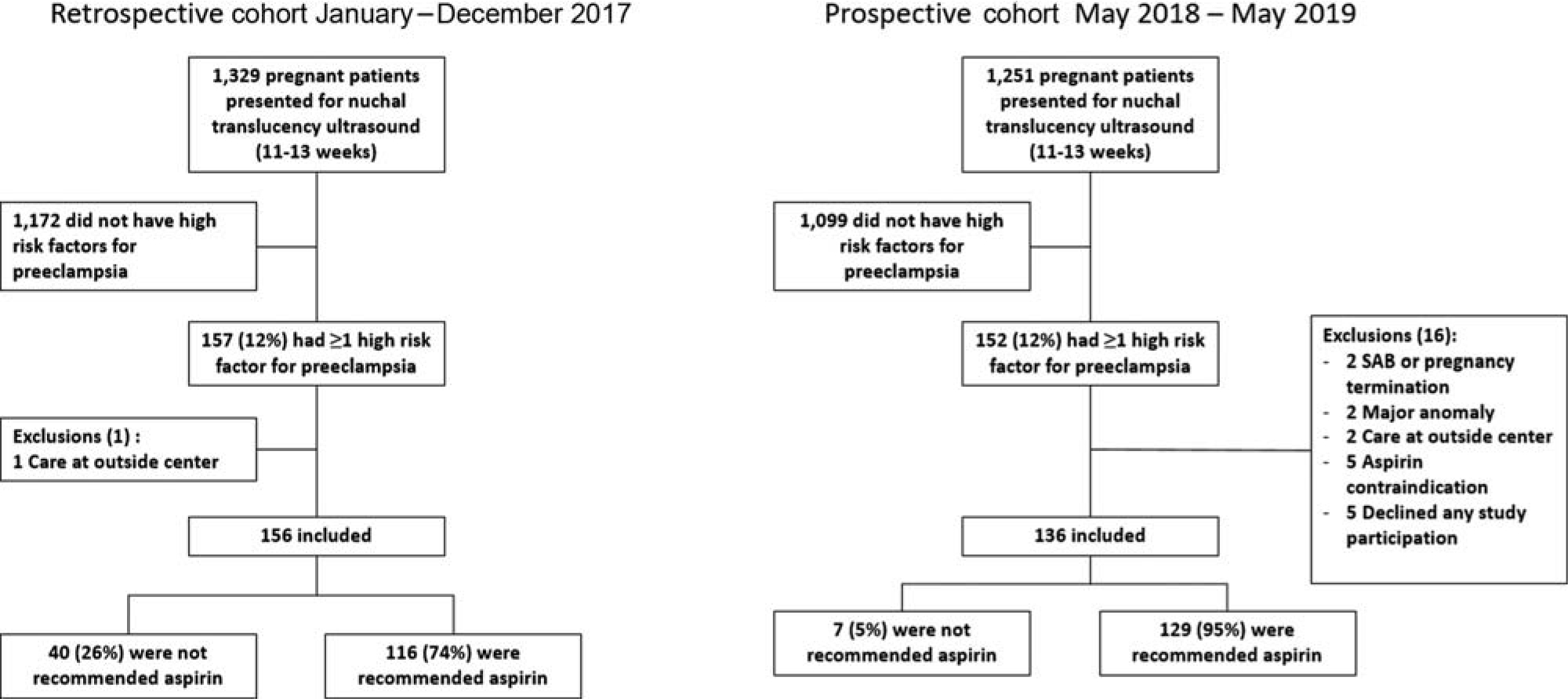
Study design: One-year prospective cohort study of patients at high risk for preeclampsia after the implementation of a screening tool (postscreen) administered to all patients at check in for NT (11-13 weeks) ultrasound. Prospective cohort was compared with one-year retrospective cohort (prescreen) the year prior (2017). All patients who presented for NT ultrasound in both cohorts were evaluated for the presence of one or more risk factor for preeclampsia with screening tool collected prospectively and chart review retrospectively. Provider recommendation for aspirin determined by documentation in prenatal record. Primary outcome was rate of provider recommendation for aspirin pre versus post screening tool, compared by Chi-square test and adjusted for potential confounders with multiple regression analysis.
Results: Pre- (n = 156) and postscreen (n = 136) cohorts were similar except for race and multifetal gestation. Prescreen, rate of provider recommendation for aspirin was 74%. Of those with prior preeclampsia, 96% were recommended aspirin, compared with 64% of patients with other risk factors (p < 0.001). Postscreen, provider recommendation of aspirin improved to 95% (p < 0.001). Rate of preeclampsia/gestational hypertension were similar between cohorts; however, there was a reduced adjusted risk in overall preterm birth <37 weeks (adjusted odds ratio [aOR] = 0.50 [0.25-0.99]) and preterm birth <34 weeks (aOR = 0.33 [0.13-0.88]) postscreening tool implementation.
Conclusion: Prior to implementation of a simple screening questionnaire, approximately 25% of high risk patients did not receive the recommendation of aspirin for preeclampsia prevention. High-risk patients who lack a history of preeclampsia were less likely to be advised of aspirin prophylaxis. Use of a simple universal screening tool at time of NT ultrasound significantly improved utilization of aspirin for preeclampsia prevention and may improve patient outcomes.
Key points: · Despite recommendations, aspirin use for preeclampsia prevention is suboptimal.. · High-risk patients who lack a history preeclampsia were less likely to be advised of aspirin use.. · A simple universal screening tool can significantly improve aspirin utilization..
Thieme. All rights reserved.
Conflict of interest statement
R.C.B. reports grants from March of Dimes Community Grant, grants from NIH (grant no.: T32GM008562), grants from PhRMA Foundation Faculty Development Award, during the conduct of the study. The other authors report no conflict of interest.
Figures


References
-
- Wong AE, Grobman WA. Medically indicated–iatrogenic prematurity. Clin Perinatol 2011;38(03):423–439 - PubMed
-
- ACOG Practice Advisory on Low-Dose Aspirin and Prevention of Preeclampsia: Updated Recommendations. Available at: http://www.losolivos-obgyn.com/info/md/acog/Low-dose%20aspirin,%20ACOG%2....Accessed December 28, 2017
-
- US Preventive Services Task Force Final recommendation statement: low-dose aspirin use for the prevention of morbidity and mortality from preeclampsia: preventive medication. Available at: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/low-....Accessed December 28, 2017
-
- ACOG Practice advisory on low dose aspirin and prevention of preeclampsia: updated recommendations. Available at: http://www.losolivos-obgyn.com/info/md/acog/Low-dose%20aspirin,%20ACOG%2....Accessed September 22, 2020
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
