

Mixed Hypertrophic and Dilated Phenotype of Cardiomyopathy in a Patient With Homozygous In-Frame Deletion in the MyBPC3 Gene Treated as Myocarditis for a Long Time
- PMID: 33101033
- PMCID: PMC7546790
- DOI: 10.3389/fphar.2020.579450
Mixed Hypertrophic and Dilated Phenotype of Cardiomyopathy in a Patient With Homozygous In-Frame Deletion in the MyBPC3 Gene Treated as Myocarditis for a Long Time
Abstract
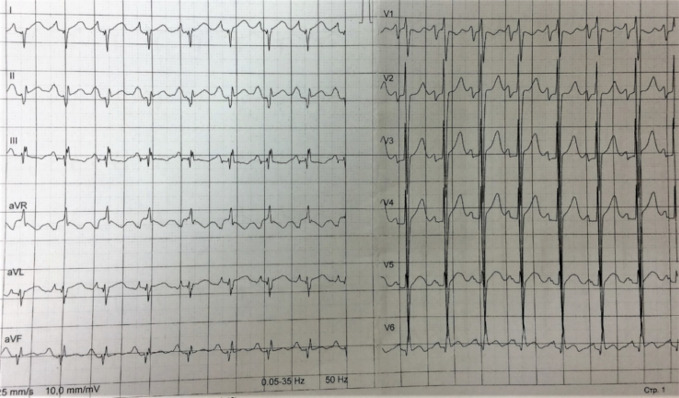
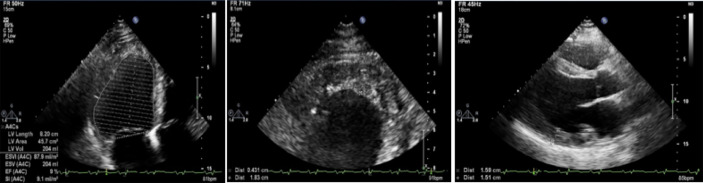
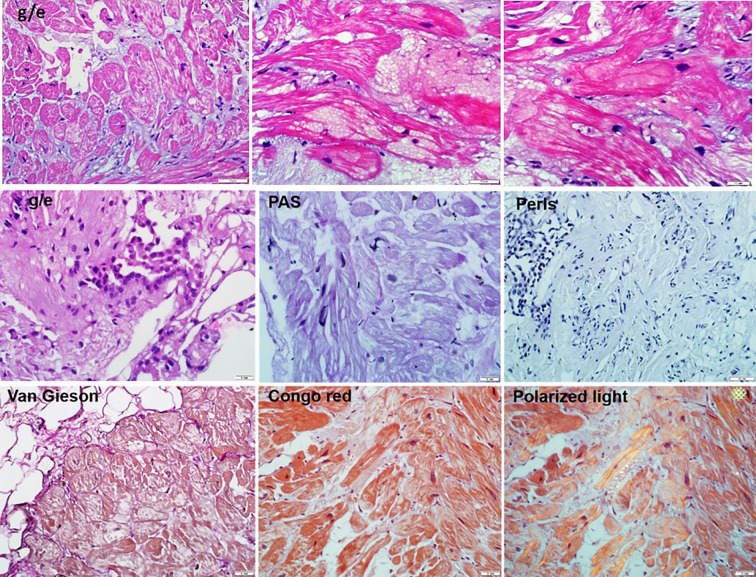
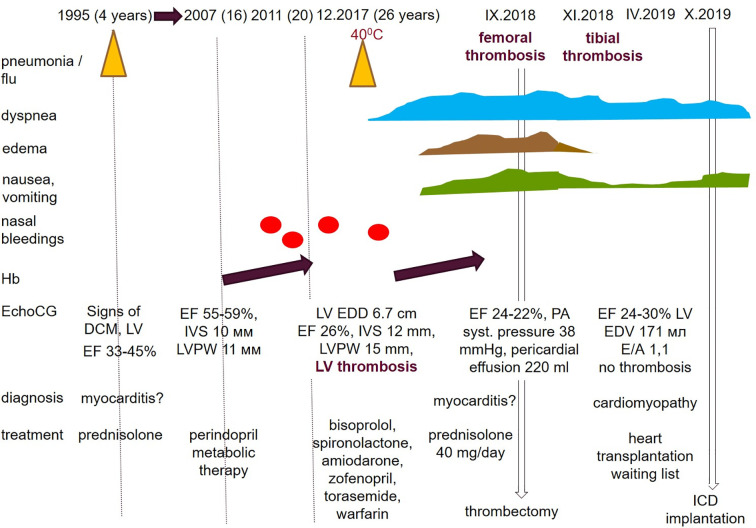
Hypertrophic cardiomyopathy (HCM) is the most common inherited disease, with a prevalence of 1:200 worldwide. The cause of HCM usually presents with an autosomal dominant mutation in the genes encoding one of more than 20 sarcomeric proteins, incomplete penetrance, and variable expressivity. HCM classically manifests as an unexplained thickness of the interventricular septum (IVS) and left ventricular (LV) walls, with or without the obstruction of the LV outflow tract (LVOT), and variable cardiac arrhythmias. Here, we present a rare case of mixed cardiomyopathy (cardiac hypertrophy and dilation) and erythrocytosis in a young patient. A 27-year-old man was admitted to the clinic due to biventricular heart failure (HF) NYHA class III. Personal medical records included a diagnosis of dilated cardiomyopathy (DCM) since the age of 4 years and were, at the time, considered an outcome of myocarditis. Severe respiratory infection led to circulatory decompensation and acute femoral thrombosis. The combination of non-obstructive LV hypertrophy (LV walls up to 15 mm), LV dilatation, decreased contractility (LV EF 24%), and LV apical thrombosis were seen. Cardiac MRI showed a complex pattern of late gadolinium enhancement (LGE). Endomyocardial biopsy (EMB) revealed primary cardiomyopathy with intravascular coagulation and an inflammatory response. No viral genome was detected in the plasma or EMB samples. Whole exome sequencing (WES) revealed a homozygous in-frame deletion p.2711_2737del in the MyBPC3 gene. The clinically unaffected mother was a heterozygous carrier of this deletion, and the father was unavailable for clinical and genetic testing. Essential erythrocytosis remains unexplained. No significant improvement was achieved by conventional treatment, including prednisolone 40 mg therapy. ICD was implanted due to sustained VT and high risk of SCD. Orthotopic heart transplantation (HTx) was considered optimal. Early manifestation combined hypertrophic and dilated phenotype, and progression may reflect a complex genotype with more than one pathogenic allele and/or a combination of genetic diseases in one patient.
Keywords: MyBPC3 gene; bi-allelic mutations; dilated cardiomyopathy; endomyocardial biopsy; heart failure progression; hypertrophic cardiomyopathy; myocarditis.
Copyright © 2020 Blagova, Alieva, Kogan, Zaytsev, Sedov, Chernyavskiy, Surikova, Kotov and Zaklyazminskaya.
Figures
Similar articles
-
Novel correlations between the genotype and the phenotype of hypertrophic and dilated cardiomyopathy: results from the German Competence Network Heart Failure.Eur J Heart Fail. 2011 Nov;13(11):1185-92. doi: 10.1093/eurjhf/hfr074. Epub 2011 Jul 12. Eur J Heart Fail. 2011. PMID: 21750094
-
[ALPK3 gene-related pediatric cardiomyopathy with craniofacial-skeletal features: a report and literature review].Zhonghua Er Ke Za Zhi. 2021 Sep 2;59(9):787-792. doi: 10.3760/cma.j.cn112140-20210222-00150. Zhonghua Er Ke Za Zhi. 2021. PMID: 34645221 Review. Chinese.
-
Long-term results of dual-chamber (DDD) pacing in obstructive hypertrophic cardiomyopathy. Evidence for progressive symptomatic and hemodynamic improvement and reduction of left ventricular hypertrophy.Circulation. 1994 Dec;90(6):2731-42. doi: 10.1161/01.cir.90.6.2731. Circulation. 1994. PMID: 7994815
-
A pathogenic nonsense mutation (c.1522C>T) of the MYBPC3 gene is implicated with hypertrophic cardiomyopathy.ESC Heart Fail. 2023 Aug;10(4):2711-2717. doi: 10.1002/ehf2.14424. Epub 2023 Jun 4. ESC Heart Fail. 2023. PMID: 37271167 Free PMC article.
-
Hypertrophic Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy.Circ Res. 2017 Sep 15;121(7):749-770. doi: 10.1161/CIRCRESAHA.117.311059. Circ Res. 2017. PMID: 28912181 Free PMC article. Review.
Cited by
-
Myocardial dysfunction caused by MyBPC3 P459fs mutation in hypertrophic cardiomyopathy: evidence from multi-omics approaches and super-resolution imaging.Front Cardiovasc Med. 2025 Feb 27;12:1529921. doi: 10.3389/fcvm.2025.1529921. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40083819 Free PMC article.
-
Humans and machines in biomedical knowledge curation: hypertrophic cardiomyopathy molecular mechanisms' representation.BioData Min. 2021 Oct 2;14(1):45. doi: 10.1186/s13040-021-00279-2. BioData Min. 2021. PMID: 34600580 Free PMC article.
References
-
- Authors/Task Force members. Elliott P. M., Anastasakis A., Borger M. A., Borggrefe M., Cecchi F., et al. (2014). ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 35 (39), 2733–2779. 10.1093/eurheartj/ehu284 - DOI - PubMed
-
- Baldi M., Sgalambro A., Nistri S., Girolami F., Baldini K., Fantini S., et al. (2010). Clinica e genetica del ventricolo sinistro non compatto: conferma di un continuum nelle cardiomiopatie [Clinical and genetic features of left ventricular noncompaction: a continuum in cardiomyopathies]. G. Ital. Cardiol. (Rome) 11 (5), 377–385. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous