

Study Protocol: The Coaching Alternative Parenting Strategies (CAPS) Study of Parent-Child Interaction Therapy in Child Welfare Families
- PMID: 33101068
- PMCID: PMC7495141
- DOI: 10.3389/fpsyt.2020.00839
Study Protocol: The Coaching Alternative Parenting Strategies (CAPS) Study of Parent-Child Interaction Therapy in Child Welfare Families
Abstract
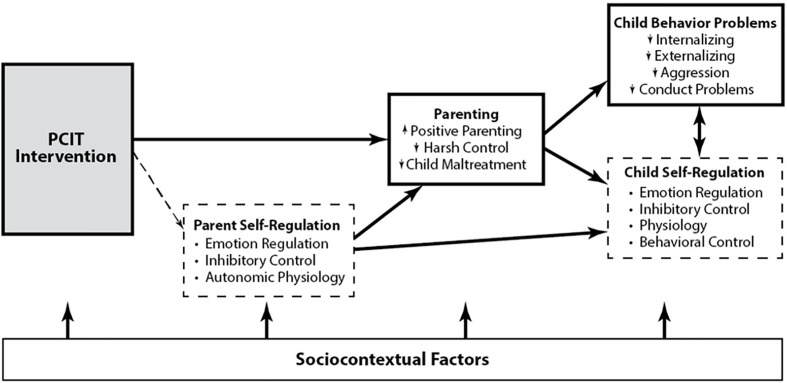
Background: Child maltreatment (CM) constitutes a serious public health problem in the United States with parents implicated in a majority of physical abuse and neglect cases. Parent-Child Interaction Therapy (PCIT) is an intensive intervention for CM families that uses innovative "bug-in-ear" coaching to improve parenting and child outcomes, and reduce CM recidivism; however, the mechanisms underlying its effects are little understood. The Coaching Alternative Parenting Strategies (CAPS) study aims to clarify the behavioral, neural, and physiological mechanisms of action in PCIT that support positive changes in parenting, improve parent and child self-regulation and social perceptions, and reduce CM in child welfare-involved families.
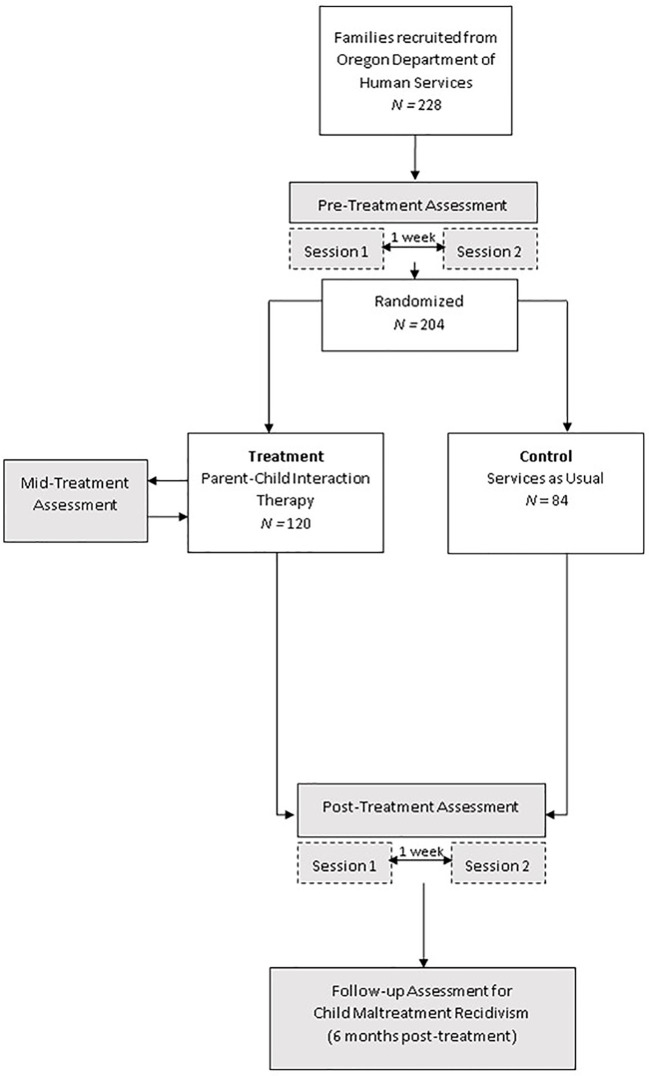
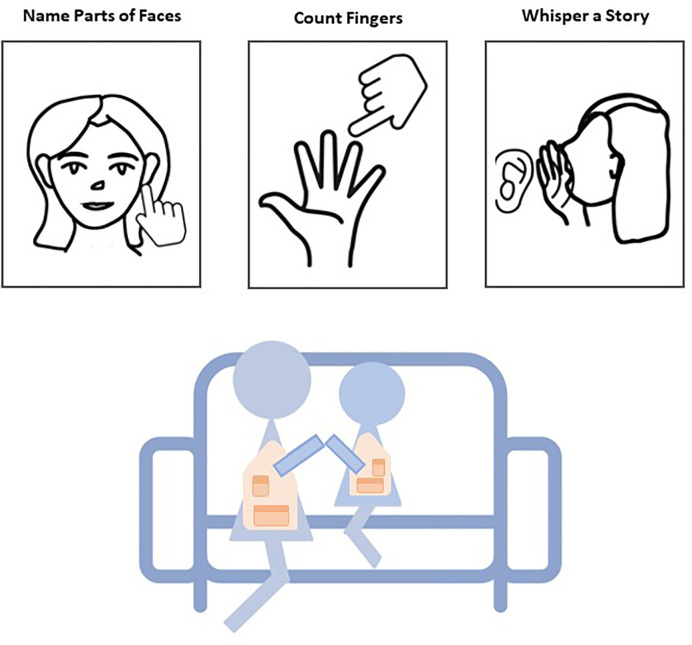
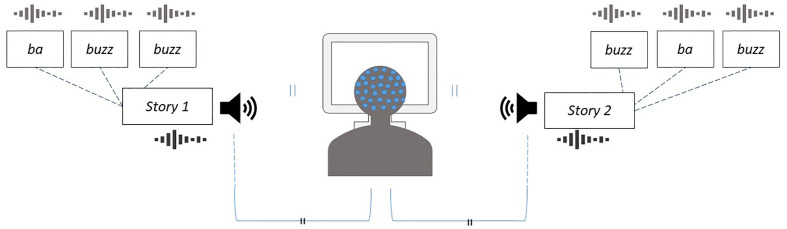
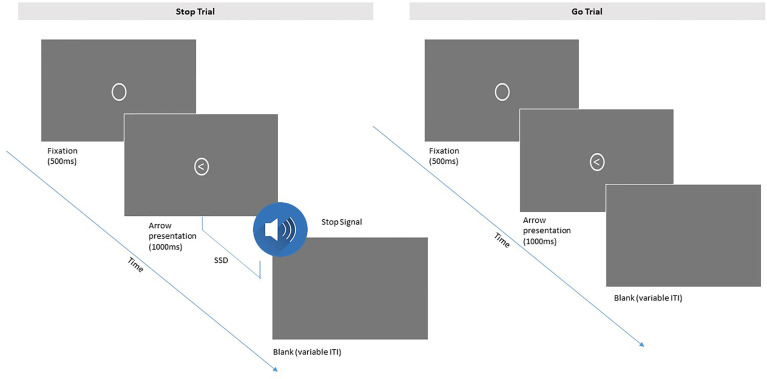
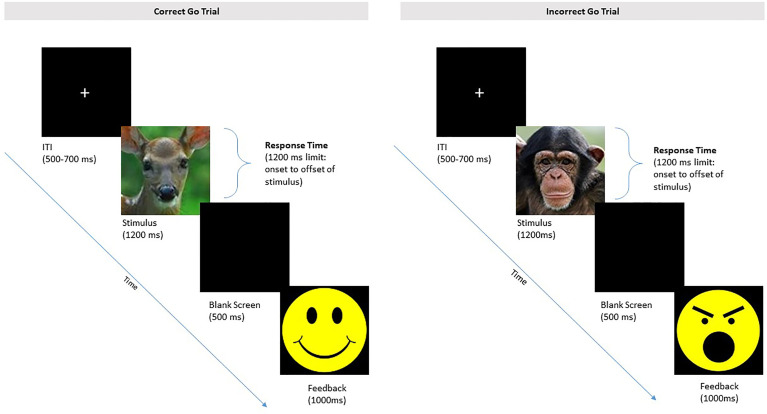
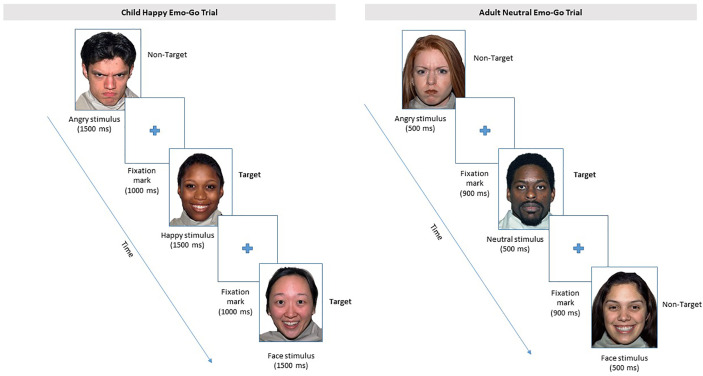
Methods: The CAPS study includes 204 child welfare-involved parent-child dyads recruited from Oregon Department of Human Services to participate in a randomized controlled trial of PCIT versus a services-as-usual control condition (clinicaltrials.gov, NCT02684903). Children ages 3-8 years at study entry and their parents complete a pre-treatment assessment prior to randomization and a post-treatment assessment 9-12 months post study entry. Dyads randomized to PCIT complete an additional, abbreviated assessment at mid-treatment. Each assessment includes individual and joint measures of parents' and children's cardiac physiology at rest, during experimental tasks, and in recovery; observational coding of parent-child interactions; and individual electroencephalogram (EEG) sessions including attentional and cognitive control tasks. In addition, parents and children complete an emotion regulation task and parents report on their own and their child's adverse childhood experiences and socio-cognitive processes, while children complete a cognitive screen and a behavioral measure of inhibitory control. Parents and children also provide anthropometric measures of allostatic load and 4-5 whole blood spots to assess inflammation and immune markers. CM recidivism is assessed for all study families at 6-month follow-up. Post-treatment and follow-up assessments are currently underway.
Discussion: Knowledge gained from this study will clarify PCIT effects on neurobehavioral target mechanisms of change in predicting CM risk reduction, positive, responsive parenting, and children's outcomes. This knowledge can help to guide efforts to tailor and adapt PCIT to vary in dosage and cost on the basis of individual differences in CM-risk factors.
Keywords: Parent-Child Interaction Therapy; cardiac physiology; child maltreatment; high density electroencephalogram; parent-child interaction; parenting; self-regulation; socio-cognitive processes.
Copyright © 2020 Nekkanti, Jeffries, Scholtes, Shimomaeda, DeBow, Norman Wells, Lyons, Giuliano, Gutierrez, Woodlee, Funderburk and Skowron.
Figures
Similar articles
-
PCIT engagement and persistence among child welfare-involved families: Associations with harsh parenting, physiological reactivity, and social cognitive processes at intake.Dev Psychopathol. 2022 Oct;34(4):1618-1635. doi: 10.1017/S0954579421000031. Epub 2021 Mar 26. Dev Psychopathol. 2022. PMID: 33766186 Free PMC article. Clinical Trial.
-
Change trajectories for parent-child interaction sequences during parent-child interaction therapy for child physical abuse.Child Abuse Negl. 2009 Jul;33(7):461-70. doi: 10.1016/j.chiabu.2008.08.003. Epub 2009 Jul 5. Child Abuse Negl. 2009. PMID: 19581001
-
A randomized controlled trial to assess the efficacy of Parenting-STAIR in treating maternal PTSD to reduce maltreatment recidivism: protocol for the Safe Mothers, Safe Children study.Trials. 2022 May 23;23(1):432. doi: 10.1186/s13063-022-06354-1. Trials. 2022. PMID: 35606818 Free PMC article.
-
Outcomes of Parent-Child Interaction Therapy (PCIT) for families presenting with child maltreatment: A systematic review.Child Abuse Negl. 2022 Dec;134:105942. doi: 10.1016/j.chiabu.2022.105942. Epub 2022 Nov 8. Child Abuse Negl. 2022. PMID: 36368165
-
Evidence-Based Treatment in Practice: PCIT Research on Addressing Individual Differences and Diversity Through the Lens of 20 Years of Service.Psychol Res Behav Manag. 2023 Jul 12;16:2599-2617. doi: 10.2147/PRBM.S360302. eCollection 2023. Psychol Res Behav Manag. 2023. PMID: 37465048 Free PMC article. Review.
Cited by
-
Randomized trial of parent-child interaction therapy improves child-welfare parents' behavior, self-regulation, and self-perceptions.J Consult Clin Psychol. 2024 Feb;92(2):75-92. doi: 10.1037/ccp0000859. Epub 2023 Dec 7. J Consult Clin Psychol. 2024. PMID: 38059943 Free PMC article. Clinical Trial.
-
Behavioral and pharmacological interventions for the prevention and treatment of psychiatric disorders with children exposed to maltreatment.Pharmacol Biochem Behav. 2021 Dec;211:173298. doi: 10.1016/j.pbb.2021.173298. Epub 2021 Nov 10. Pharmacol Biochem Behav. 2021. PMID: 34774585 Free PMC article. Review.
-
Infant Parent Support (IPS): a multidisciplinary intervention to improve the mental health of children with a social worker - a study protocol for a feasibility randomised controlled trial with embedded process evaluation.Pilot Feasibility Stud. 2025 Jun 5;11(1):78. doi: 10.1186/s40814-025-01616-6. Pilot Feasibility Stud. 2025. PMID: 40474316 Free PMC article.
-
In vivo social regulation of high-risk parenting: A conceptual model of Parent-Child Interaction Therapy for child maltreatment prevention.Child Youth Serv Rev. 2022 May;136:106391. doi: 10.1016/j.childyouth.2022.106391. Epub 2022 Jan 31. Child Youth Serv Rev. 2022. PMID: 35221407 Free PMC article.
-
A Digital Microintervention Supporting Evidence-Based Parenting Skills: Development Study Using the Agile Scrum Methodology.JMIR Form Res. 2024 Jun 28;8:e54892. doi: 10.2196/54892. JMIR Form Res. 2024. PMID: 38941594 Free PMC article.
References
-
- Skowron E, Reinemann DH. Effectiveness of psychological interventions for child maltreatment: A meta-analysis. Psychother: Theory Res Pract Training (2005) 42(1):52–71. 10.1037/0033-3204.42.1.52 - DOI
-
- U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau Child Maltreatment 2011. Washington, DC: US Government Printing Office; (2012). Available from: http://www.acf.hhs.gov/programs/cb/research-data-technology/statistics-r....
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous