

Inflammation, Thrombosis, and Destruction: The Three-Headed Cerberus of Trauma- and SARS-CoV-2-Induced ARDS
- PMID: 33101314
- PMCID: PMC7546394
- DOI: 10.3389/fimmu.2020.584514
Inflammation, Thrombosis, and Destruction: The Three-Headed Cerberus of Trauma- and SARS-CoV-2-Induced ARDS
Abstract
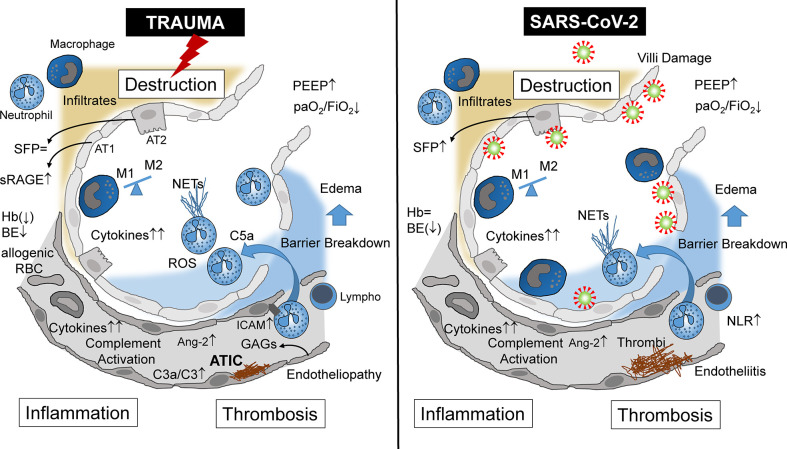
Physical trauma can be considered an unrecognized "pandemic" because it can occur anywhere and affect anyone and represents a global burden. Following severe tissue trauma, patients frequently develop acute lung injury (ALI) and/or acute respiratory distress syndrome (ARDS) despite modern surgical and intensive care concepts. The underlying complex pathophysiology of life-threatening ALI/ARDS has been intensively studied in experimental and clinical settings. However, currently, the coronavirus family has become the focus of ALI/ARDS research because it represents an emerging global public health threat. The clinical presentation of the infection is highly heterogeneous, varying from a lack of symptoms to multiple organ dysfunction and mortality. In a particular subset of patients, the primary infection progresses rapidly to ALI and ARDS. The pathophysiological mechanisms triggering and driving severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-induced ALI/ARDS are still poorly understood. Although it is also generally unknown whether insights from trauma-induced ARDS may be readily translated to SARS-CoV-2-associated ARDS, it was still recommended to treat coronavirus-positive patients with ALI/ARDS with standard protocols for ALI/ARDS. However, this strategy was questioned by clinical scientists, because it was documented that some severely hypoxic SARS-CoV-2-infected patients exhibited a normal respiratory system compliance, a phenomenon rarely observed in ARDS patients with another underlying etiology. Therefore, coronavirus-induced ARDS was defined as a specific ARDS phenotype, which accordingly requires an adjusted therapeutic approach. These suggestions reflect previous attempts of classifying ARDS into different phenotypes that might overall facilitate ARDS diagnosis and treatment. Based on the clinical data from ARDS patients, two major phenotypes have been proposed: hyper- and hypo-inflammatory. Here, we provide a comparative review of the pathophysiological pathway of trauma-/hemorrhagic shock-induced ARDS and coronavirus-induced ARDS, with an emphasis on the crucial key points in the pathogenesis of both these ARDS forms. Therefore, the manifold available data on trauma-/hemorrhagic shock-induced ARDS may help to better understand coronavirus-induced ARDS.
Keywords: acute respiratory distress syndrome; lung; pathophysiology; severe acute respiratory syndrome coronavirus 2; trauma.
Copyright © 2020 Lupu, Palmer and Huber-Lang.
Figures
Similar articles
-
Emerging Mechanisms of Pulmonary Vasoconstriction in SARS-CoV-2-Induced Acute Respiratory Distress Syndrome (ARDS) and Potential Therapeutic Targets.Int J Mol Sci. 2020 Oct 29;21(21):8081. doi: 10.3390/ijms21218081. Int J Mol Sci. 2020. PMID: 33138181 Free PMC article. Review.
-
Highlight of Immune Pathogenic Response and Hematopathologic Effect in SARS-CoV, MERS-CoV, and SARS-Cov-2 Infection.Front Immunol. 2020 May 12;11:1022. doi: 10.3389/fimmu.2020.01022. eCollection 2020. Front Immunol. 2020. PMID: 32574260 Free PMC article. Review.
-
A Mouse-Adapted SARS-CoV-2 Induces Acute Lung Injury and Mortality in Standard Laboratory Mice.Cell. 2020 Nov 12;183(4):1070-1085.e12. doi: 10.1016/j.cell.2020.09.050. Epub 2020 Sep 23. Cell. 2020. PMID: 33031744 Free PMC article.
-
[Comparison of clinical and pathological features between severe acute respiratory syndrome and coronavirus disease 2019].Zhonghua Jie He He Hu Xi Za Zhi. 2020 Jun 12;43(6):496-502. doi: 10.3760/cma.j.cn112147-20200311-00312. Zhonghua Jie He He Hu Xi Za Zhi. 2020. PMID: 32241072 Chinese.
-
Remdesivir against COVID-19 and Other Viral Diseases.Clin Microbiol Rev. 2020 Oct 14;34(1):e00162-20. doi: 10.1128/CMR.00162-20. Print 2020 Dec 16. Clin Microbiol Rev. 2020. PMID: 33055231 Free PMC article. Review.
Cited by
-
One Year On: Are We Ready for COVID?Arch Bronconeumol (Engl Ed). 2021 Mar 13;57(8):517-8. doi: 10.1016/j.arbres.2021.02.016. Online ahead of print. Arch Bronconeumol (Engl Ed). 2021. PMID: 33795187 Free PMC article. English, Spanish. No abstract available.
-
Ultrastructural examination of lung "cryobiopsies" from a series of fatal COVID-19 cases hardly revealed infected cells.Virchows Arch. 2022 May;480(5):967-977. doi: 10.1007/s00428-022-03308-5. Epub 2022 Mar 16. Virchows Arch. 2022. PMID: 35294603 Free PMC article.
-
Association between trauma exposure and respiratory disease-A Mendelian randomization study.Front Endocrinol (Lausanne). 2022 Sep 5;13:1001223. doi: 10.3389/fendo.2022.1001223. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36133309 Free PMC article.
-
Simulation of COVID-19 symptoms in a genetically engineered mouse model: implications for the long haulers.Mol Cell Biochem. 2023 Jan;478(1):103-119. doi: 10.1007/s11010-022-04487-0. Epub 2022 Jun 22. Mol Cell Biochem. 2023. PMID: 35731343 Free PMC article.
-
The hemostatic activity and Mechanistic roles of glucosyloxybenzyl 2-isobutylmalate extract (BSCE) from Bletilla striata (Thunb.) Rchb.f. in Inhibiting pulmonary hemorrhage.Heliyon. 2024 Sep 20;10(18):e38203. doi: 10.1016/j.heliyon.2024.e38203. eCollection 2024 Sep 30. Heliyon. 2024. PMID: 39381249 Free PMC article.
References
-
- World Health Organisation (WHO) Injuries and Violence: the facts. (2014). p. 1–20. Available at: https://www.who.int/violence_injury_prevention/media/news/2015/Injury_vi....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous