

Laparoscopic Partial Splenectomy Assisted by Fluorescence in a 13-Year-Old Girl
- PMID: 33101836
- PMCID: PMC7577790
- DOI: 10.1055/s-0040-1716894
Laparoscopic Partial Splenectomy Assisted by Fluorescence in a 13-Year-Old Girl
Abstract
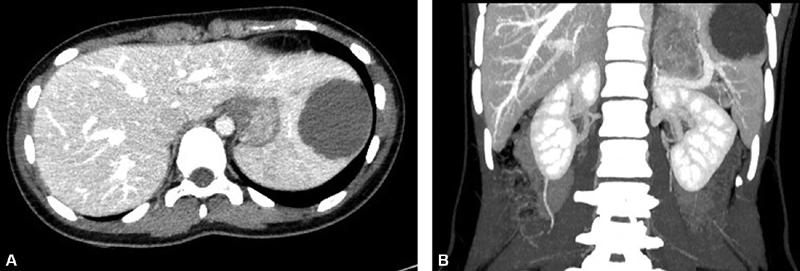
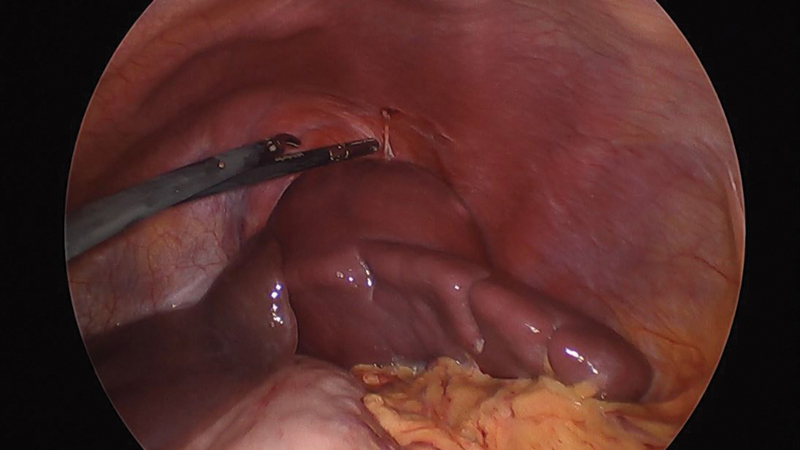
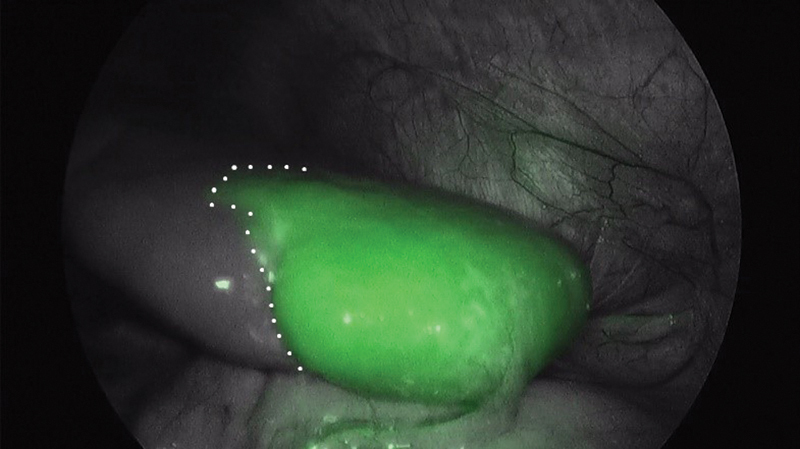
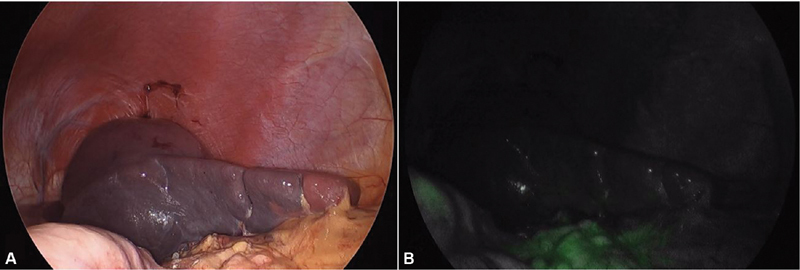
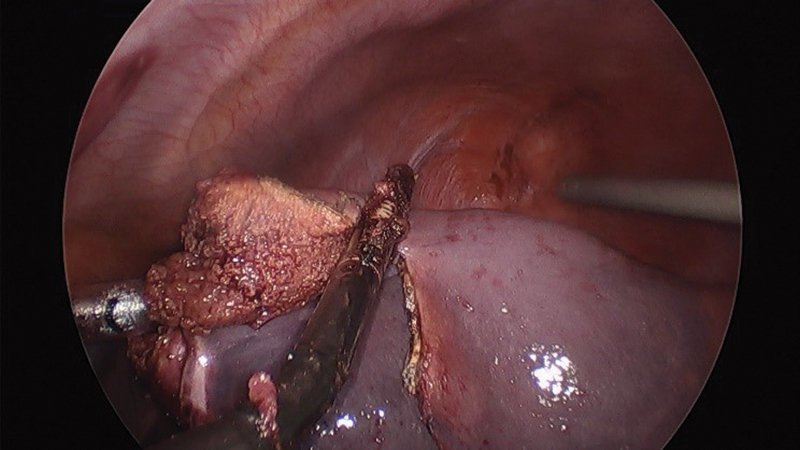
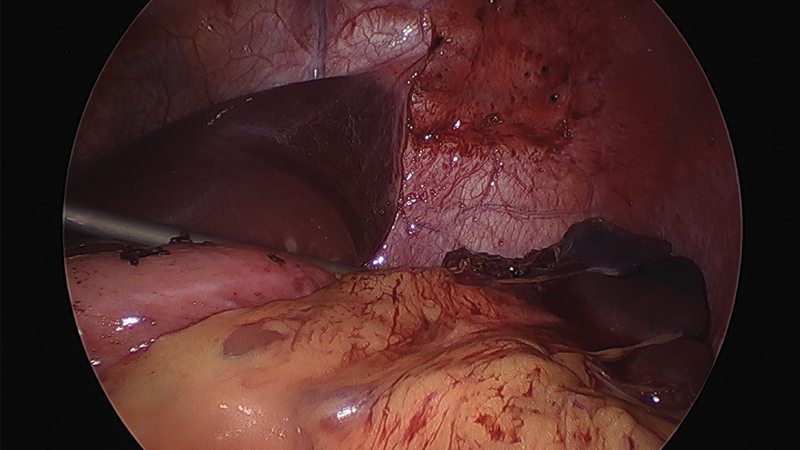
Partial splenectomy allows preserving immune function in benign splenic lesions such as epidermoid cysts. Determining the plane of resection and perfusion of the spleen remnant can be difficult, especially in centrally located lesions. We present a 13-year-old girl with a symptomatic splenic cyst of 6 cm in diameter located next to the splenic hilum. Laparoscopic partial splenectomy was performed through a 10-mm umbilical approach and three accessory 5-mm ports. Intraoperative intravenous injection of indocyanine green (ICG) at 0.2 mg/kg guided the careful dissection of the splenic hilum and checked the spleen perfusion once the upper arterial branch was clamped. The subsequent wash-out of the ICG allowed inspection of the peripheral vascular return of the splenic remnant through polar veins. Surgery was uneventful with minimal blood loss. Follow-up ultrasound scan revealed a well-perfused small splenic remnant with no signs of recurrence. Laparoscopic partial splenectomy is feasible in benign splenic tumors, especially in those cases of peripheral location. Fluorescence facilitates the safe dissection of the splenic hilum, the visualization of the transection plane of the spleen and the perfusion of the remnant in cases of anatomically and technically complicated partial splenectomies.
Keywords: fluorescence; indocyanine green; laparoscopy; partial splenectomy; pediatric.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. ( https://creativecommons.org/licenses/by/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures
References
-
- Boybeyi O, Karnak I, Tanyel F C, Ciftçi A O, Senocak M E. The management of primary nonparasitic splenic cysts. Turk J Pediatr. 2010;52(05):500–504. - PubMed
-
- Kenney C D, Hoeger Y E, Yetasook A K. Management of non-parasitic splenic cysts: does size really matter? J Gastrointest Surg. 2014;18(09):1658–1663. - PubMed
-
- Chen Y Y, Shyr Y M, Wang S E. Epidermoid cyst of the spleen. J Gastrointest Surg. 2013;17(03):555–561. - PubMed
Publication types
LinkOut - more resources
Full Text Sources