

Prostatic artery embolization versus transurethral resection of the prostate in management of benign prostatic hyperplasia
- PMID: 33102395
- PMCID: PMC7557197
- DOI: 10.1016/j.prnil.2020.04.001
Prostatic artery embolization versus transurethral resection of the prostate in management of benign prostatic hyperplasia
Abstract
Background: Transurethral resection of the prostate (TURP) is considered the gold standard surgical intervention for prostate size less than 80 g. Prostatic artery embolization (PAE) has been suggested as a minimally invasive interventional radiological procedure in the management of benign prostatic hyperplasia (BPH), especially by using the PErFecTED technique. We aim through our study to evaluate the efficacy and safety of PAE compared with those of monopolar transurethral resection of prostate (M-TURP) and bipolar transurethral resection of prostate (B-TURP) in treating lower urinary tract symptoms (LUTSs) secondary to BPH.
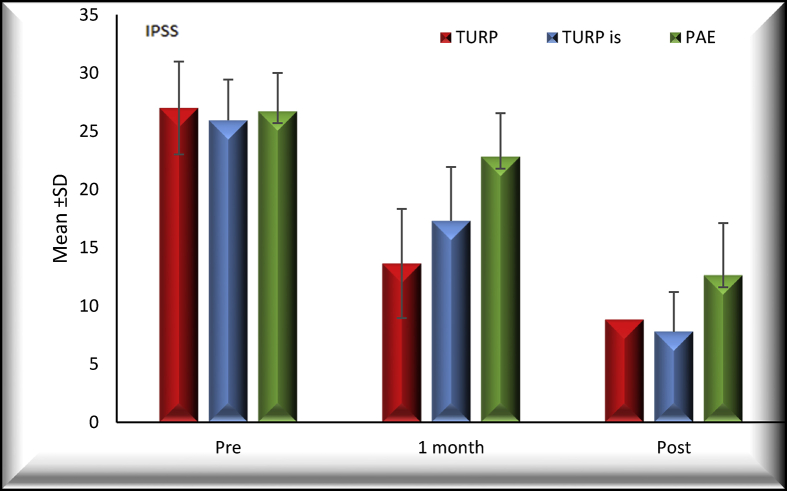
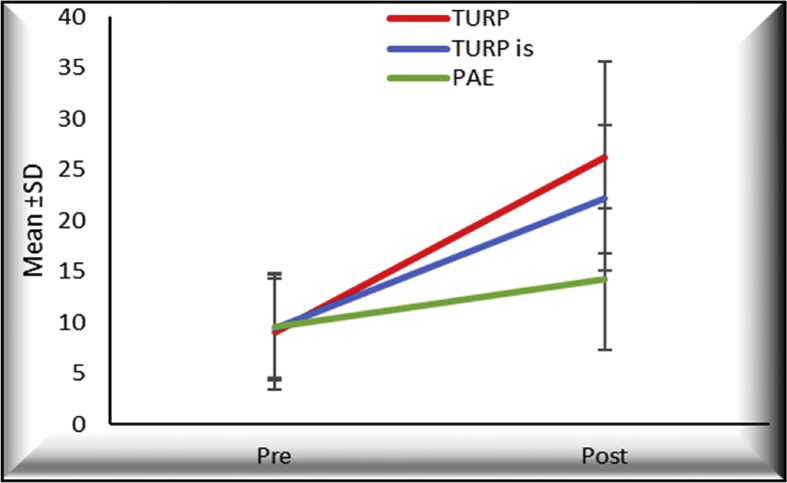
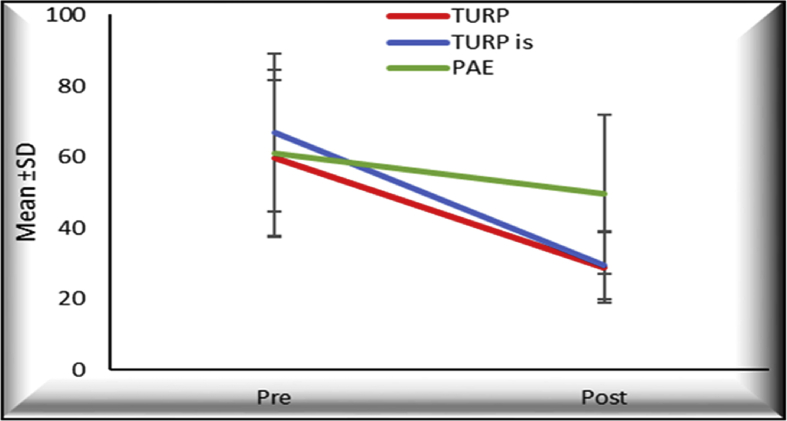
Methods: We randomized 60 patients into 3 equal groups representing M-TURP, B-TURP, and PAE. Patients were followed up at 1 and 6 months postoperatively with regard to the International prostate symptom score (IPSS) score; uroflowmetry; prostate volume by transrectal ultrasound; and postvoid residual urine.
Results: The mean operative time was 59, 68, and 89 minutes for the M-TURP group, the B-TURP group, and the PAE group, respectively; only one patient, who represented 5% of the M-TURP group and 1.7% of the whole study population, developed transurethral resection syndrome. Four patients of the PAE group complained of postembolization syndrome, which represented 20% of the cases. Only two patients in our study, both belonging to the PAE group, developed acute urinary retention after catheter removal, representing 10% of the PAE group and 3.33% of the whole study population. The improvement in the IPSS score, the average uroflowmetry (Q-average) score, postvoid residual urine, and prostate volume reduction was noted in all groups, with more statistically significant improvement in each of the M-TURP and the B-TURP groups than in the PAE group.
Conclusion: PErFecTED technique is a novel way of embolization, with statistically significant improvement for patients complaining of LUTSs due to BPH in terms of improvement of IPSS, uroflowmetry, prostate size, and amount of postvoid residual urine, yet these results are still not comparable with either the results of M-TURP or B-TURP that still show more effective improvement.
Keywords: Embolization; IPSS; LUTS; Prostate; TURP; Urine retention.
© 2020 Asian Pacific Prostate Society. Published by Elsevier B.V.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Gravas S., Cornu J.N., Drake M.J., Gacci CG M., Herrmann T.R.W., Madersbacher CM S. EAU Guidelines Panel on Treatment of Non-neurogenic Male LUTS Guidelines: Management of Non-Neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Obstruction (BPO) Eur Assoc Urol. 2018;36(4):575–584. doi: 10.1007/s00345-018-2220-z. http://uroweb.org/wp-content/uploads/EAU-Guidelines-on-the-Management-of... - DOI
-
- Avins A.L., Barry M.J., Bruskewitz R.C., Donnell R.F., Foster H.E., Gonzalez C.M. BPH); 2010. American Urological Association Guideline: Management of Benign Prostatic Hyperplasia (BPH) AUA Staff: Chapter 1: Guideline on the Management of Benign Prostatic Hyperplasia.
LinkOut - more resources
Full Text Sources