

The Role of Prognostic and Predictive Biomarkers for Assessing Cardiovascular Risk in Chronic Kidney Disease Patients
- PMID: 33102575
- PMCID: PMC7568793
- DOI: 10.1155/2020/2314128
The Role of Prognostic and Predictive Biomarkers for Assessing Cardiovascular Risk in Chronic Kidney Disease Patients
Abstract
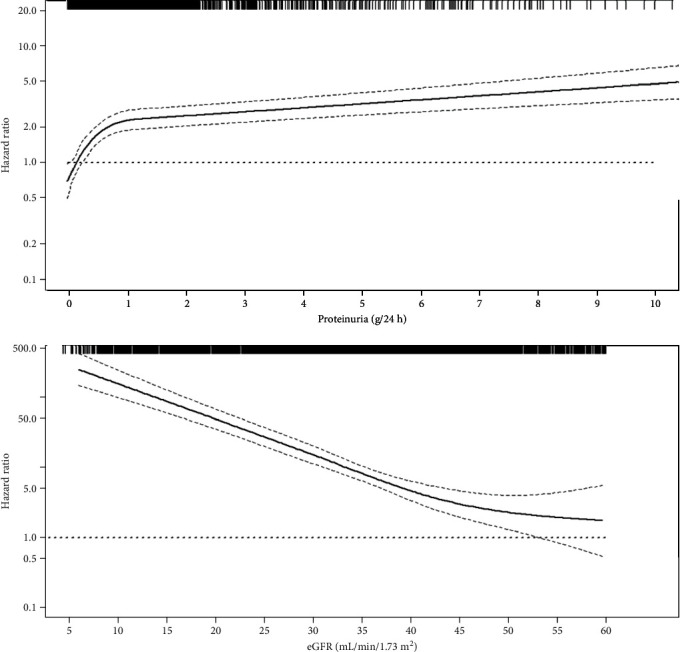
Chronic kidney disease (CKD) is currently defined as the presence of proteinuria and/or an eGFR < 60 mL/min/1.73m2 on the basis of the renal diagnosis. The global dimension of CKD is relevant, since its prevalence and incidence have doubled in the past three decades worldwide. A major complication that occurs in CKD patients is the development of cardiovascular (CV) disease, being the incidence rate of fatal/nonfatal CV events similar to the rate of ESKD in CKD. Moreover, CKD is a multifactorial disease where multiple mechanisms contribute to the individual prognosis. The correct development of novel biomarkers of CV risk may help clinicians to ameliorate the management of CKD patients. Biomarkers of CV risk in CKD patients are classifiable as prognostic, which help to improve CV risk prediction regardless of treatment, and predictive, which allow the selection of individuals who are likely to respond to a specific treatment. Several prognostic (cystatin C, cardiac troponins, markers of inflammation, and fibrosis) and predictive (genes, metalloproteinases, and complex classifiers) biomarkers have been developed. Despite previous biomarkers providing information on the pathophysiological mechanisms of CV risk in CKD beyond proteinuria and eGFR, only a minority have been adopted in clinical use. This mainly depends on heterogeneous results and lack of validation of biomarkers. The purpose of this review is to present an update on the already assessed biomarkers of CV risk in CKD and examine the strategies for a correct development of biomarkers in clinical practice. Development of both predictive and prognostic biomarkers is an important task for nephrologists. Predictive biomarkers are useful for designing novel clinical trials (enrichment design) and for better understanding of the variability in response to the current available treatments for CV risk. Prognostic biomarkers could help to improve risk stratification and anticipate diagnosis of CV disease, such as heart failure and coronary heart disease.
Copyright © 2020 Michele Provenzano et al.
Conflict of interest statement
The authors declare they have no conflict of interests.
Figures
References
-
- KidneyDiseaseImproving Global Outcomes Work Group. Chapter 4: other complications of CKD: CVD, medication dosage, patient safety, infections, hospitalizations, and caveats for investigating complications of CKD. Kidney International. Supplement. 2013;3(1):91–111. doi: 10.1038/kisup.2012.67. - DOI - PMC - PubMed
-
- Roth G. A., Abate D., Abate K. H., et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017 [published correction appears in Lancet. 2019 Jun 22; 393(10190):e44] [published correction appears in Lancet. 2018 Nov 17; 392(10160):2170] The Lancet. 2018;392(10159):1736–1788. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
