

Quality of Care for Acute Kidney Disease: Current Knowledge Gaps and Future Directions
- PMID: 33102955
- PMCID: PMC7569680
- DOI: 10.1016/j.ekir.2020.07.031
Quality of Care for Acute Kidney Disease: Current Knowledge Gaps and Future Directions
Abstract
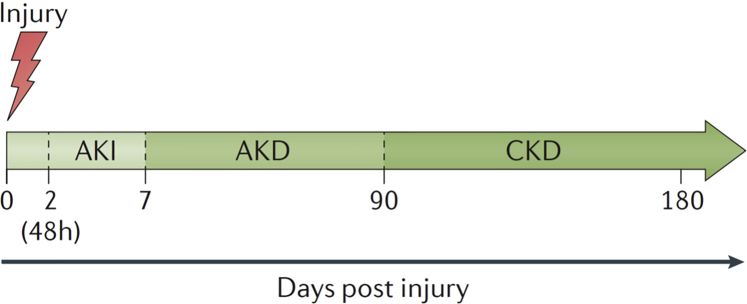
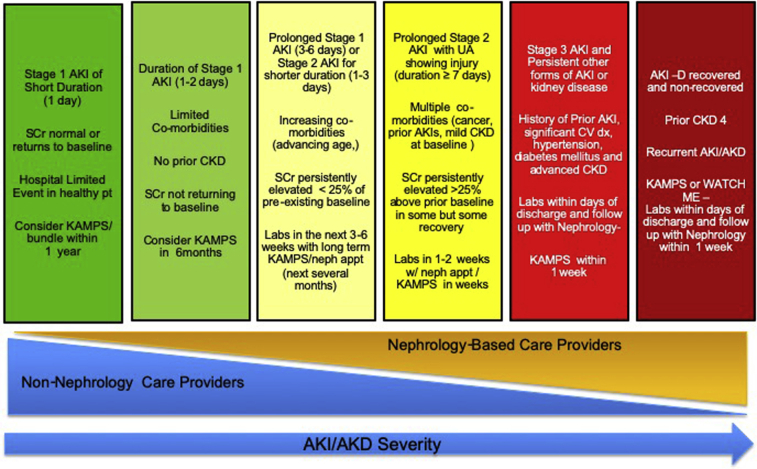
Acute kidney injury (AKI) and acute kidney disease (AKD) are common complications in hospitalized patients and are associated with adverse outcomes. Although consensus guidelines have improved the care of patients with AKI and AKD, guidance regarding quality metrics in the care of patients after an episode of AKI or AKD is limited. For example, few patients receive follow-up laboratory testing of kidney function or post-AKI or AKD care through nephrology or other providers. Recently, the Acute Disease Quality Initiative developed a consensus statement regarding quality improvement goals for patients with AKI or AKD specifically highlighting efforts regarding quality and safety of care after hospital discharge after an episode of AKI or AKD. The goal is to use these measures to identify opportunities for improvement that will positively affect outcomes. We recommend that health care systems quantitate the proportion of patients who need and actually receive follow-up care after the index AKI or AKD hospitalization. The intensity and appropriateness of follow-up care should depend on patient characteristics, severity, duration, and course of AKI of AKD, and should evolve as evidence-based guidelines emerge. Quality indicators for discharged patients with dialysis requiring AKI or AKD should be distinct from end-stage renal disease measures. Besides, there should be specific quality indicators for those still requiring dialysis in the outpatient setting after AKI or AKD. Given the limited preexisting data guiding the care of patients after an episode of AKI or AKD, there is ample opportunity to establish quality measures and potentially improve patient care and outcomes. This review will provide specific evidence-based and expert opinion-based guidance for the care of patients with AKI or AKD after hospital discharge.
Keywords: acute kidney injury; outcomes; quality; recovery.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures
Similar articles
-
Recovery Dynamics and Prognosis After Dialysis for Acute Kidney Injury.JAMA Netw Open. 2024 Mar 4;7(3):e240351. doi: 10.1001/jamanetworkopen.2024.0351. JAMA Netw Open. 2024. PMID: 38457183 Free PMC article.
-
Acute kidney disease in hospitalized acute kidney injury patients.PeerJ. 2021 May 24;9:e11400. doi: 10.7717/peerj.11400. eCollection 2021. PeerJ. 2021. PMID: 34113486 Free PMC article.
-
Acute kidney disease and long-term outcomes in critically ill acute kidney injury patients with sepsis: a cohort analysis.Clin Kidney J. 2020 Sep 27;14(5):1379-1387. doi: 10.1093/ckj/sfaa130. eCollection 2021 May. Clin Kidney J. 2020. PMID: 33959267 Free PMC article.
-
Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup.Nat Rev Nephrol. 2017 Apr;13(4):241-257. doi: 10.1038/nrneph.2017.2. Epub 2017 Feb 27. Nat Rev Nephrol. 2017. PMID: 28239173
-
Defining AKD: The Spectrum of AKI, AKD, and CKD.Nephron. 2022;146(3):302-305. doi: 10.1159/000516647. Epub 2021 Jun 24. Nephron. 2022. PMID: 34167119 Review.
Cited by
-
Posthospital Multidisciplinary Care for AKI Survivors: A Feasibility Pilot.Kidney Med. 2023 Oct 5;5(12):100734. doi: 10.1016/j.xkme.2023.100734. eCollection 2023 Dec. Kidney Med. 2023. PMID: 37964784 Free PMC article.
-
Assessment of Acute Kidney Injury and Longitudinal Kidney Function After Hospital Discharge Among Patients With and Without COVID-19.JAMA Netw Open. 2021 Mar 1;4(3):e211095. doi: 10.1001/jamanetworkopen.2021.1095. JAMA Netw Open. 2021. PMID: 33688965 Free PMC article.
-
Transitions of dialysis status and outcomes after the unplanned first dialysis: a nationwide population-based cohort study.Sci Rep. 2023 Aug 8;13(1):12867. doi: 10.1038/s41598-023-39913-w. Sci Rep. 2023. PMID: 37553351 Free PMC article.
-
Holistic Patient-Centered Outcomes in Post-Acute Kidney Injury Care: Physical, Emotional, Cognitive, and Social Outcomes.Adv Kidney Dis Health. 2025 Mar;32(2):162-178. doi: 10.1053/j.akdh.2024.10.001. Adv Kidney Dis Health. 2025. PMID: 40222803 Review.
-
Identification and outcomes of acute kidney disease in patients presenting in Bolivia, Brazil, South Africa, and Nepal.PLoS Med. 2024 Nov 14;21(11):e1004495. doi: 10.1371/journal.pmed.1004495. eCollection 2024 Nov. PLoS Med. 2024. PMID: 39541400 Free PMC article.
References
-
- Chertow G.M., Burdick E., Honour M. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16:3365–3370. - PubMed
-
- Gocze I., Jauch D., Gotz M. Biomarker-guided intervention to prevent acute kidney injury after major surgery: the prospective randomized BigpAK study. Ann Surg. 2018;267:1013–1020. - PubMed
