

IgA Nephropathy Genetic Risk Score to Estimate the Prevalence of IgA Nephropathy in UK Biobank
- PMID: 33102956
- PMCID: PMC7572308
- DOI: 10.1016/j.ekir.2020.07.012
IgA Nephropathy Genetic Risk Score to Estimate the Prevalence of IgA Nephropathy in UK Biobank
Abstract
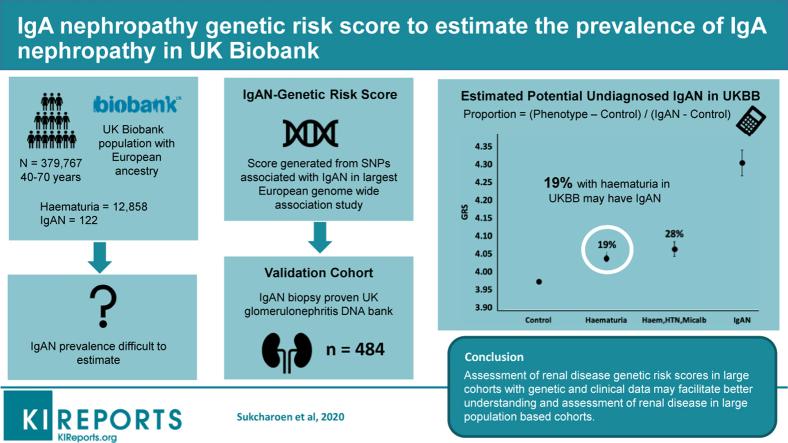
Background: IgA nephropathy (IgAN) is the commonest glomerulonephritis worldwide. Its prevalence is difficult to estimate, as people with mild disease do not commonly receive a biopsy diagnosis. We aimed to generate an IgA nephropathy genetic risk score (IgAN-GRS) and estimate the proportion of people with hematuria who had IgAN in the UK Biobank (UKBB).
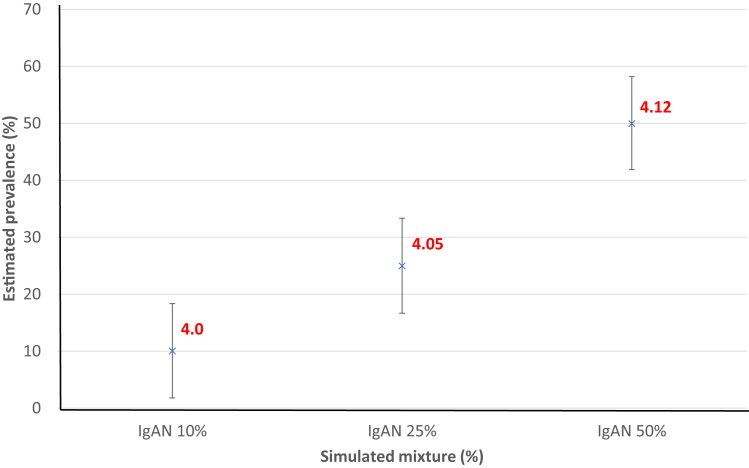
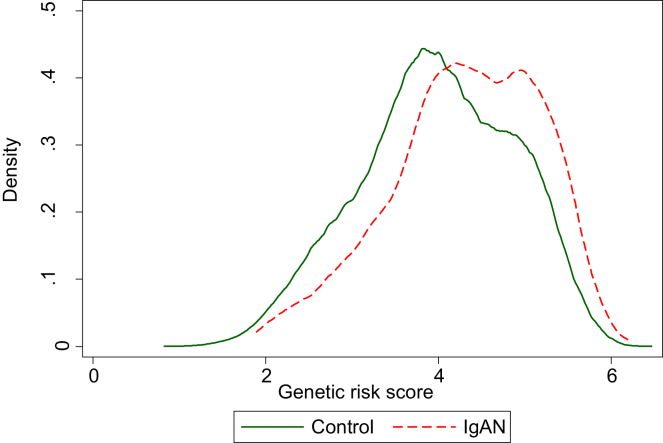
Methods: We calculated an IgAN-GRS using 14 single-nucleotide polymorphisms (SNPs) drawn from the largest European Genome-Wide Association Study (GWAS) and validated the IgAN-GRS in 464 biopsy-proven IgAN European cases from the UK Glomerulonephritis DNA Bank (UKGDB) and in 379,767 Europeans in the UKBB. We used the mean of IgAN-GRS to calculate the proportion of potential IgAN in 14,181 with hematuria and other nonspecific renal phenotypes from 379,767 Europeans in the UKBB.
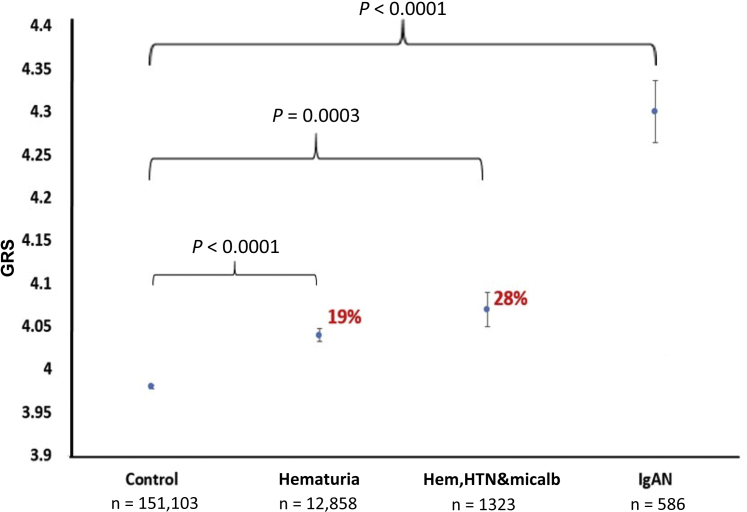
Results: The IgAN-GRS was higher in the IgAN cohort (4.30; 95% confidence interval [95% CI: 4.23-4.38) than in controls (3.98; 3.97-3.98; P < 0.0001). The mean GRS in UKBB participants with hematuria (n = 12,858) was higher (4.04; 4.02-4.06) than UKBB controls (3.98; 3.97-3.98; P < 0.0001) and higher in those with hematuria, hypertension, and microalbuminuria (n = 1323) (4.07; 4.02-4.13) versus (3.98; 3.97-3.98; P = 0.0003). Using the difference in these means, we estimated that IgAN accounted for 19% of noncancer hematuria and 28% with hematuria, hypertension, and microalbuminuria in UKBB.
Conclusions: We used an IgAN-GRS to estimate the prevalence of IgAN contributing to common phenotypes that are not always biopsied. The noninvasive use of polygenic risk in this setting may have further utility to identify likely etiology of nonspecific renal phenotypes in large population cohorts.
Keywords: Genetic Risk Scores; IgA nephropathy; chronic kidney disease; epidemiology; hematuria.
Crown Copyright © 2020 Published by Elsevier Inc. on behalf of the International Society of Nephrology.
Figures
Comment in
-
IgAN Genetic Risk Score in the Clinical Setting.Kidney Int Rep. 2020 Aug 5;5(10):1627-1629. doi: 10.1016/j.ekir.2020.07.032. eCollection 2020 Oct. Kidney Int Rep. 2020. PMID: 33104093 Free PMC article. No abstract available.
References
-
- Schena F., Nistor I. Epidemiology of IgA nephropathy: a global perspective. Semin Nephrol. 2018;38:435–442. - PubMed
-
- McGrogan A., Franssen C., de Vries C. The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. Nephrol Dial Transplant. 2010;26:414–430. - PubMed
-
- Donadio J., Grande J. IgA nephropathy. N Engl J Med. 2002;347:738–748. - PubMed
-
- Barratt J. IgA nephropathy. J Am Soc Nephrol. 2005;16:2088–2097. - PubMed
-
- Imai E., Yamagata K., Iseki K. Kidney disease screening program in Japan: history, outcome, and perspectives. Clin J Am Soc Nephrol. 2007;2:1360–1366. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
