

Influence of Strongyloides stercoralis Coinfection on the Presentation, Pathogenesis, and Outcome of Tuberculous Meningitis
- PMID: 33104201
- PMCID: PMC9071290
- DOI: 10.1093/infdis/jiaa672
Influence of Strongyloides stercoralis Coinfection on the Presentation, Pathogenesis, and Outcome of Tuberculous Meningitis
Abstract
Background: Helminth infections may modulate the inflammatory response to Mycobacterium tuberculosis and influence disease presentation and outcome. Strongyloides stercoralis is common among populations with high tuberculosis prevalence. Our aim was to determine whether S. stercoralis coinfection influenced clinical presentation, cerebrospinal fluid (CSF) inflammation, and outcome from tuberculous meningitis (TBM).
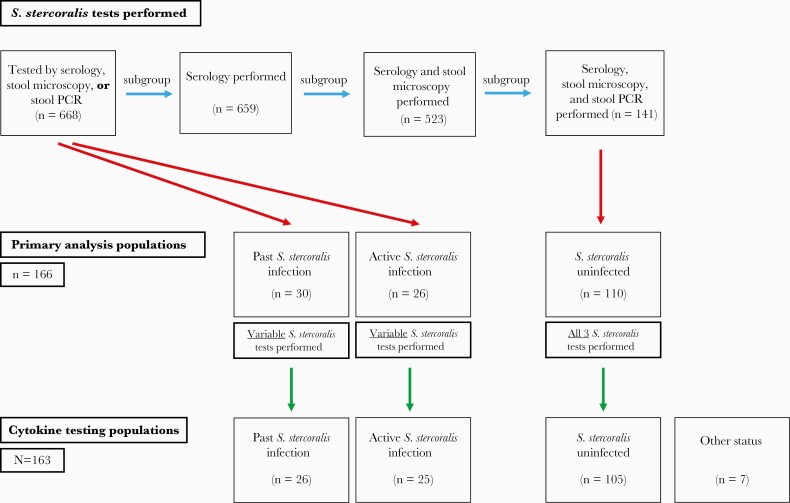
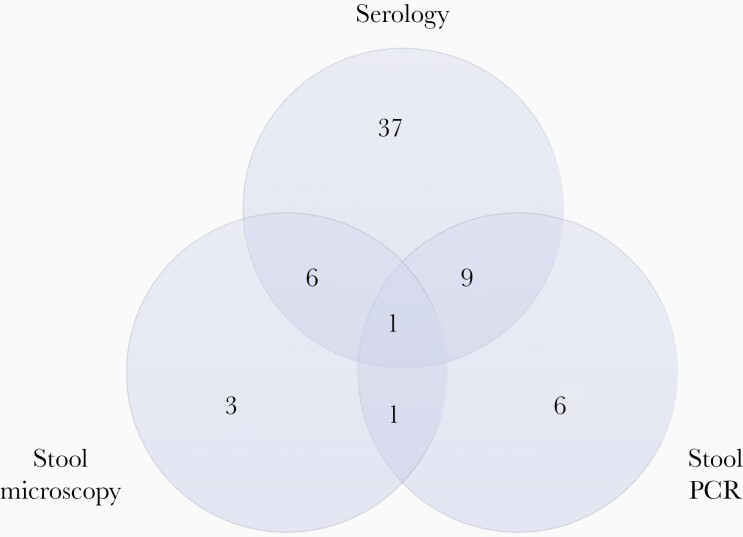
Methods: From June 2017 to December 2019, 668 Vietnamese adults with TBM, enrolled in the ACT HIV or LAST ACT trials (NCT03092817 and NCT03100786), underwent pretreatment S. stercoralis testing by serology, stool microscopy, and/or stool polymerase chain reaction. Comparisons of pretreatment TBM severity, CSF inflammation (including cytokines), and 3-month clinical end points were performed in groups with or without active S. stercoralis infection.
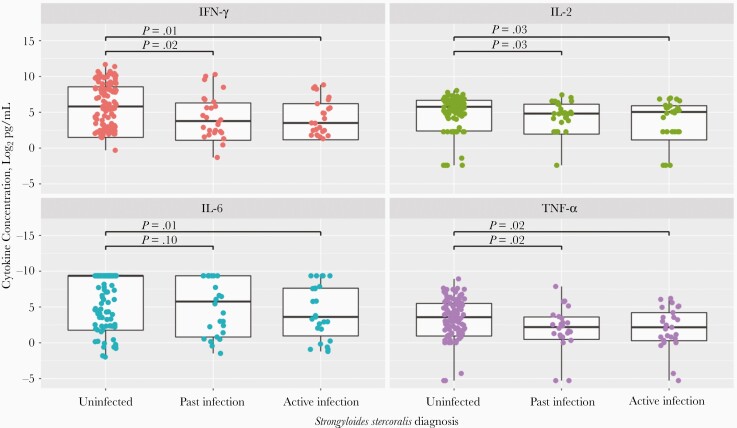
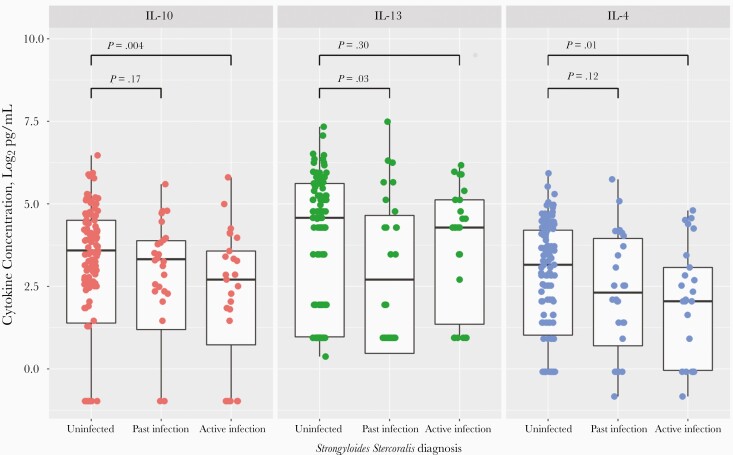
Results: Overall, 9.4% participants (63 of 668) tested positive for S. stercoralis. Active S. stercoralis infection was significantly associated with reduced pretreatment CSF neutrophil counts (median [interquartile range], 3/μL [0-25/μL] vs 14 /μL [1-83/μL]; P = .04), and with reduced CSF interferon ɣ, interleukin 2, and tumor necrosis factor α concentrations (11.4 vs 56.0 pg/mL [P = .01], 33.1 vs 54.5 pg/mL [P = .03], and 4.5 vs 11.9 pg/mL [P = .02], respectively), compared with uninfected participants. Neurological complications by 3 months were significantly reduced in participants with active S. stercoralis infection compared with uninfected participants (3.8% [1 of 26] vs 30.0% [33 of 110], respectively; P = .01).
Conclusions: S. stercoralis coinfection may modulate the intracerebral inflammatory response to M. tuberculosis and improve TBM clinical outcomes.
Keywords: Strongyloides stercoralis; cytokines; immunomodulation; inflammation; outcome; tuberculous meningitis.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- World Health Organization. Strongyloidiasis. World Health Organization; 2016. http://www.who.int/intestinal_worms/epidemiology/strongyloidiasis/en/. Accessed 26 June 2020.
-
- Thwaites GE, Bang ND, Dung NH, et al. . Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults. N Engl J Med 2004; 351:1741–51. - PubMed
-
- Ruslami R, Ganiem AR, Dian S, et al. . Intensified regimen containing rifampicin and moxifloxacin for tuberculous meningitis: an open-label, randomised controlled phase 2 trial. Lancet Infect Dis 2013; 13:27–35. - PubMed
