

Effect of an Electronic Health Record "Nudge" on Opioid Prescribing and Electronic Health Record Keystrokes in Ambulatory Care
- PMID: 33105005
- PMCID: PMC7878599
- DOI: 10.1007/s11606-020-06276-1
Effect of an Electronic Health Record "Nudge" on Opioid Prescribing and Electronic Health Record Keystrokes in Ambulatory Care
Abstract
Background: Multiple policy initiatives encourage more cautious prescribing of opioids in light of their risks. Electronic health record (EHR) redesign can influence prescriber choices, but some redesigns add to workload.
Objective: To estimate the effect of an EHR prescribing redesign on both opioid prescribing choices and keystrokes.
Design: Quality improvement quasi-experiment, analyzed as interrupted time series.
Participants: Adult patients of an academic multispecialty practice and a federally qualified health center (FQHC) who received new prescriptions for short-acting opioids, and their providers.
Intervention: In the redesign, new prescriptions of short-acting opioids defaulted to the CDC-recommended minimum for opioid-naïve patients, with no alerts or hard stops, such that 9 keystrokes were required for a guideline-concordant prescription and 24 for a non-concordant prescription.
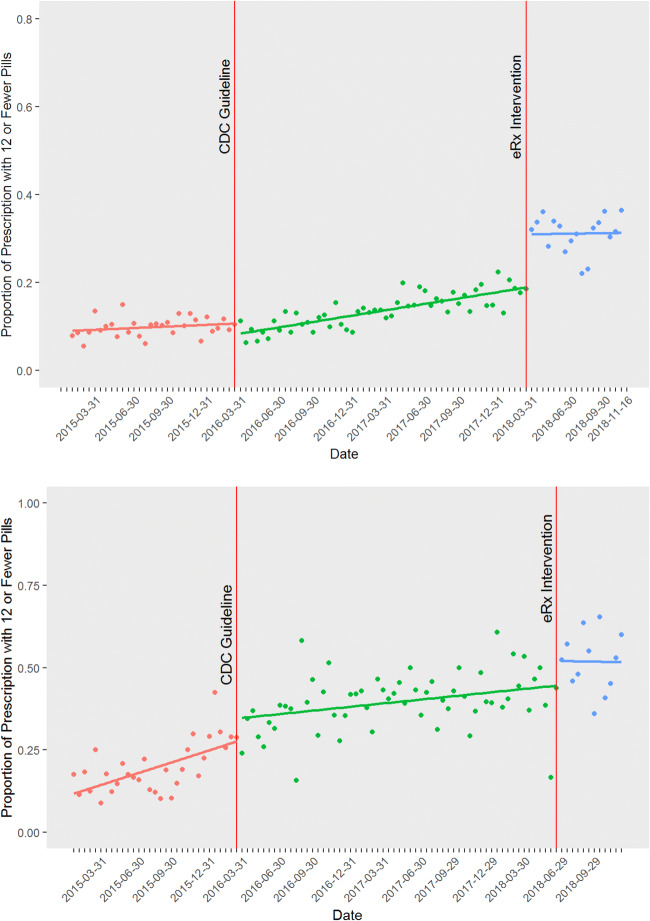
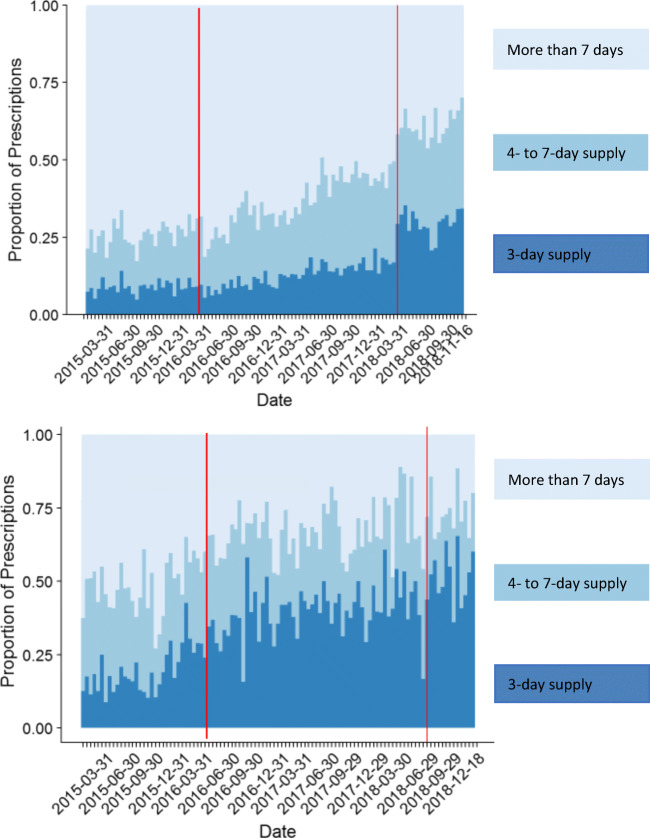
Main measures: Proportion of guideline-concordant prescriptions, defined as new prescriptions with a 3-day supply or less, calculated per 2-week period. Number of mouse clicks and keystrokes needed to place prescriptions.
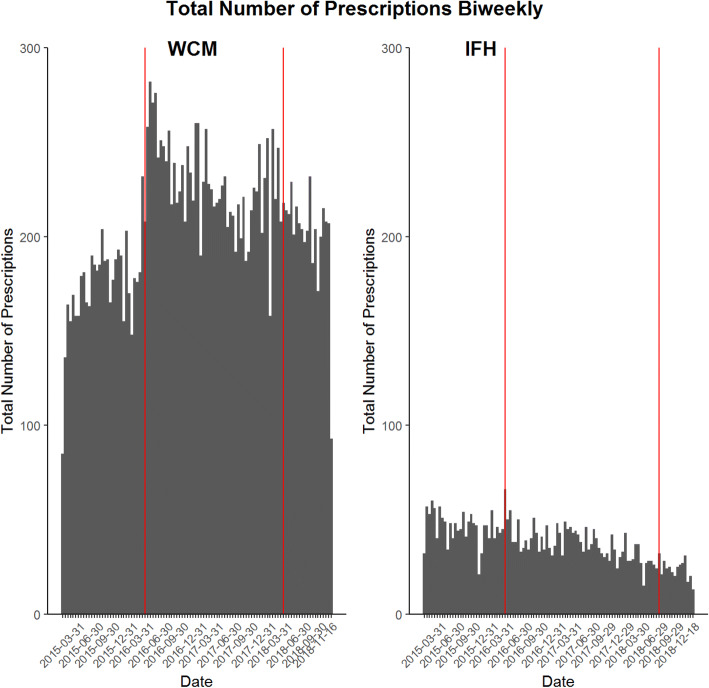
Key results: Across the 2 sites, 22,113 patients received a new short-acting opioid prescription from 821 providers. Before the intervention, both settings showed secular trends toward smaller-quantity prescriptions. At the academic practice, the intervention was associated with an immediate increase in guideline-concordant prescriptions from an average of 12% to 31% of all prescriptions. At the FQHC, about 44% of prescriptions were concordant at the time of the intervention, which was not associated with an additional significant increase. However, total keystrokes needed to place the concordant prescriptions decreased 62.7% from 3552 in the 6 months before the intervention to 1323 in the 6 months afterwards.
Conclusions: Autocompleting prescription forms with guideline-recommended values was associated with a large increase in guideline concordance in an organization where baseline concordance was low, but not in an organization where it was already high. The redesign markedly reduced the number of keystrokes needed to place orders, with important implications for EHR-related stress.
Trial registration: www.ClinicalTrials.gov protocol 1710018646.
Keywords: EHR workload; behavioral nudge; clinical decision support; electronic health records; electronic prescribing; opioid prescribing.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Centers for Disease Control and Prevention, National Center for Health Statistics. Number and age-adjusted rates of drug-poisoning deaths involving opioid analgesics and heroin: United States, 2000-2014. National Vital Statistics System, Mortality File. Atlanta (GA).
-
- Centers for Disease Control and Prevention. Increases in fentanyl drug confiscations and fentanyl-related overdose fatalities. CDC Health Advisory. 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
