

Can Upstream Patient Education Improve Fracture Care in a Digital World? Use of a Decision Aid for the Treatment of Displaced Diaphyseal Clavicle Fractures
- PMID: 33105455
- PMCID: PMC7887007
- DOI: 10.1097/BOT.0000000000001916
Can Upstream Patient Education Improve Fracture Care in a Digital World? Use of a Decision Aid for the Treatment of Displaced Diaphyseal Clavicle Fractures
Abstract
Background: The increasing proportion of telemedicine and virtual care in orthopaedic surgery presents an opportunity for upstream delivery of patient facing tools, such as decision aids. Displaced diaphyseal clavicle fractures (DDCFs) are ideal for a targeted intervention because there is no superior treatment, and decisions are often dependent on patient's preference. A decision aid provided before consultation may educate a patient and minimize decisional conflict similarly to inperson consultation with an orthopaedic traumatologist.
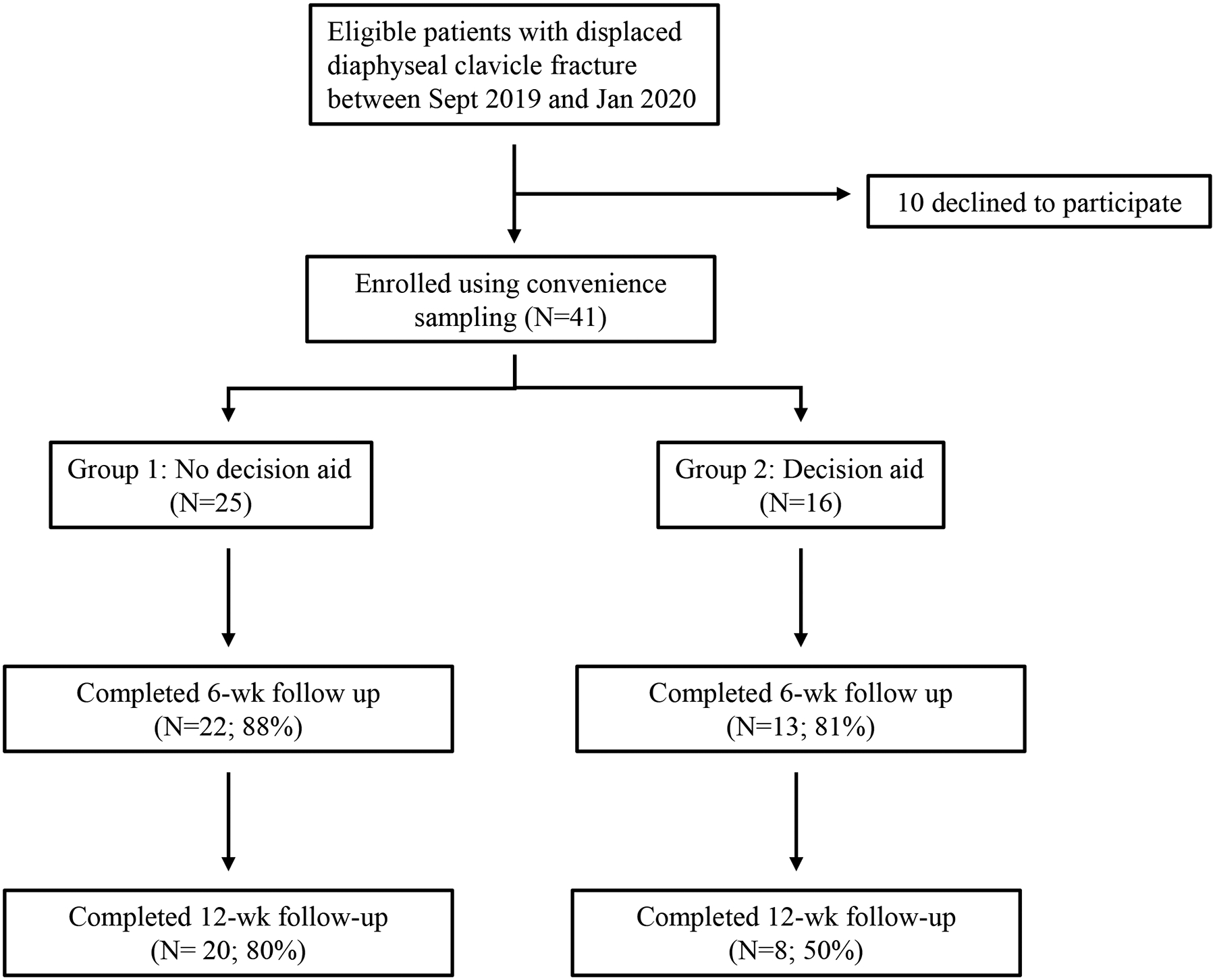
Methods: Patients with DDCF were enrolled into 2 groups. The usual care group participated in a discussion with a trauma fellowship-trained orthopaedic surgeon. Patients in the intervention group were administered a DDCF decision aid designed with the International Patient Decision Aid Standards. Primary comparisons were made based on a decisional conflict score. Secondary outcomes included treatment choice, pain score, QuickDASH, and opinion toward cosmetic appearance.
Results: A total of 41 patients were enrolled. Decisional conflict scores were similar and low between the 2 groups: 11.8 (usual care) and 11.4 (decision aid). There were no differences in secondary outcomes between usual care and the decision aid.
Discussion: Our decision aid for the management of DDCF produces a similarly low decisional conflict score to consultation with an orthopaedic trauma surgeon. This decision aid could be a useful resource for surgeons who infrequently treat this injury or whose practices are shifting toward telemedicine visits. Providing a decision aid before consultation may help incorporate patient's values and preferences into the decision-making process between surgery and nonoperative management.
Level of evidence: Therapeutic Level II. See Instructions for Authors for a complete description of levels of evidence.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
M. R. DeBaun is the recipient of a grant from the Orthopaedic Trauma Association and the Stanford Clinical and Translational Science Award (CTSA) to Spectrum (UL1 TR001085). The CTSA program is led by the National Center for Advancing Translational Sciences (NCATS) at the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. The remaining authors report no conflict of interest.
Figures

References
-
- Rowell PD, Pincus P, White M, et al. Telehealth in paediatric orthopaedic surgery in Queensland: a 10-year review. ANZ J Surg. 2014;84:955–959. - PubMed
-
- Buvik A, Bugge E, Knutsen G, et al. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25:451–459. - PubMed
-
- Lambrecht CJ, Canham WD, Gattey PH, et al. Telemedicine and orthopaedic care. A review of 2 years of experience. Clin Orthop Relat Res. 1998:228–232. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
