

Pharmacoresistant Epilepsy in Childhood: Think of the Cerebral Folate Deficiency, a Treatable Disease
- PMID: 33105619
- PMCID: PMC7690394
- DOI: 10.3390/brainsci10110762
Pharmacoresistant Epilepsy in Childhood: Think of the Cerebral Folate Deficiency, a Treatable Disease
Abstract
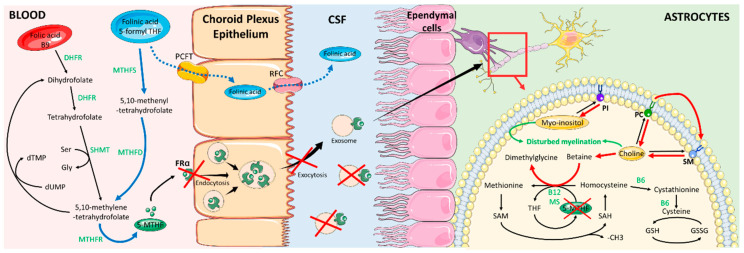
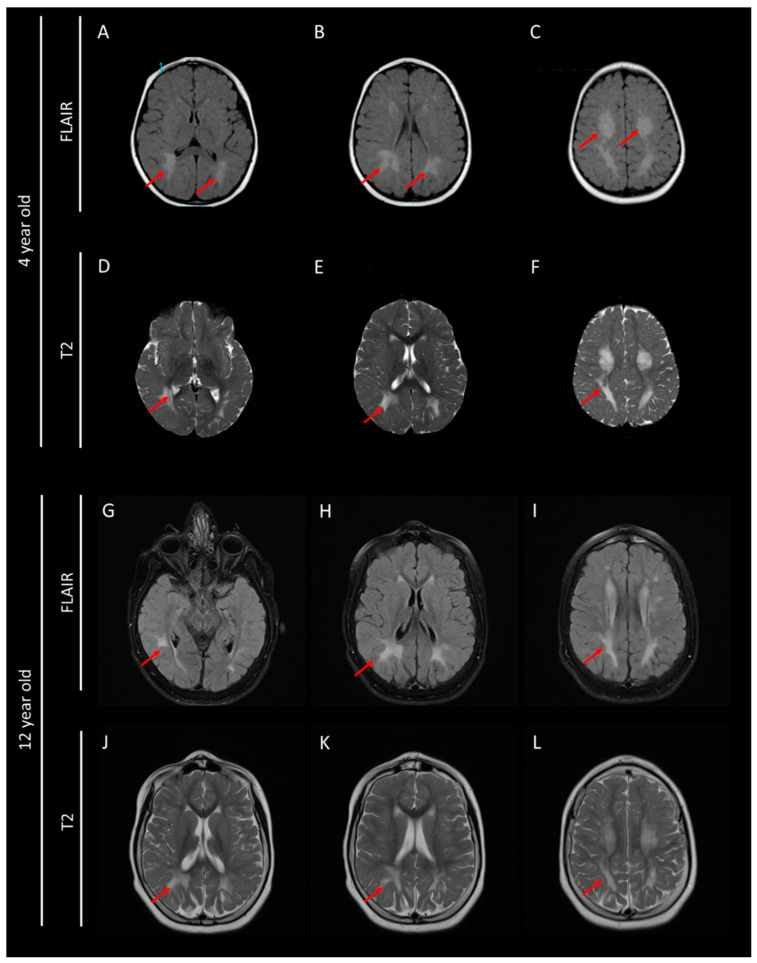
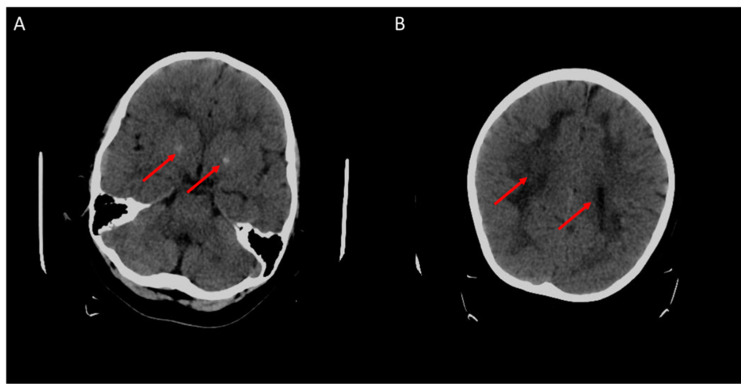
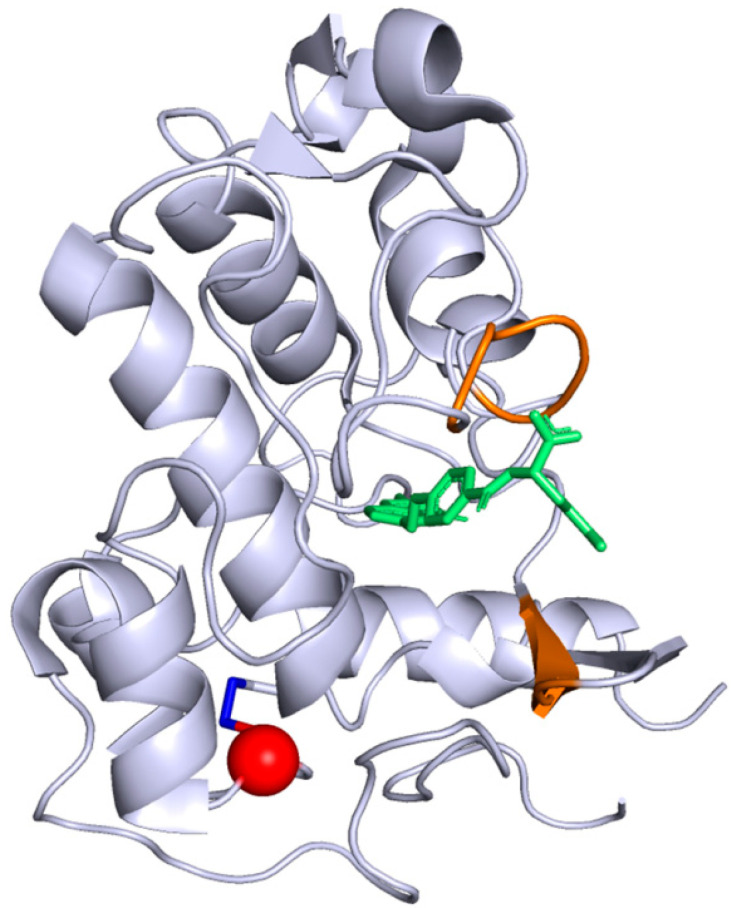
Cerebral folate deficiency (CFD) is a neurological disorder characterized by low levels of 5-methyltetrahydrofolate (5-MTHF) in the cerebrospinal fluid (CSF). The prevalence of this autosomal recessive disorder is estimated to be <1/1,000,000. Fifteen different pathogenic variants in the folate receptor 1 gene (FOLR1) encoding the receptor of folate α (FRα) have already been described. We present a new pathogenic variation in the FOLR1 in a childhood-stage patient. We aim to establish the core structure of the FRα protein mandatory for its activity. A three-year-old child was admitted at hospital for a first febrile convulsions episode. Recurrent seizures without fever also occurred a few months later, associated with motor and cognitive impairment. Various antiepileptic drugs failed to control seizures. Magnetic resonance imaging (MRI) showed central hypomyelination and biological analysis revealed markedly low levels of 5-MTHF in CSF. Next generation sequencing (NGS) confirmed a CFD with a FOLR1 homozygous variation (c.197 G > A, p.Cys66Tyr). This variation induces an altered folate receptor α protein and underlines the role of a disulfide bond: Cys66-Cys109, essential to transport 5-MTHF into the central nervous system. Fortunately, this severe form of CFD had remarkably responded to high doses of oral folinic acid combined with intravenous administrations.
Keywords: FOLR1 variant; FRα protein crystallographic structure; cerebral folate deficiency; epilepsy; neurodegenerative disorder; pediatric.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Frewin R. Clinical Biochemistry: Metabolic and Clinical Aspects: Third Edition. Churchill Livingstone, Elsevier; London, UK: 2014. Biochemical aspects of anaemia; pp. 515–532.
-
- Cario H., Smith D.E.C., Blom H., Blau N., Bode H., Holzmann K., Pannicke U., Hopfner K.P., Rump E.M., Ayric Z., et al. Dihydrofolate reductase deficiency due to a homozygous DHFR mutation causes megaloblastic anemia and cerebral folate deficiency leading to severe neurologic disease. Am. J. Hum. Genet. 2011;88:226–231. doi: 10.1016/j.ajhg.2011.01.007. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
