

Title: Cytokine release syndrome is not usually caused by secondary hemophagocytic lymphohistiocytosis in a cohort of 19 critically ill COVID-19 patients
- PMID: 33106497
- PMCID: PMC7589537
- DOI: 10.1038/s41598-020-75260-w
Title: Cytokine release syndrome is not usually caused by secondary hemophagocytic lymphohistiocytosis in a cohort of 19 critically ill COVID-19 patients
Abstract
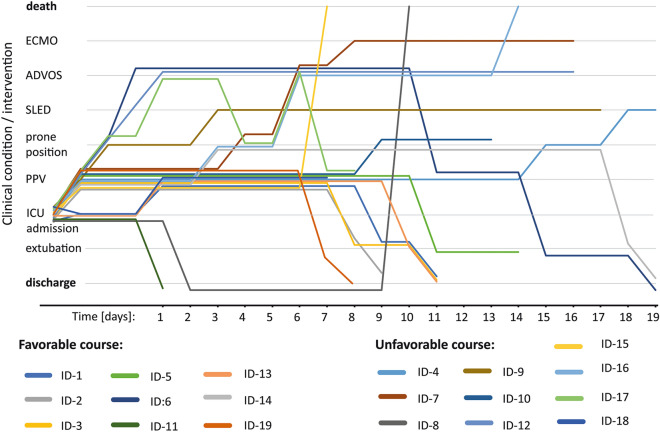
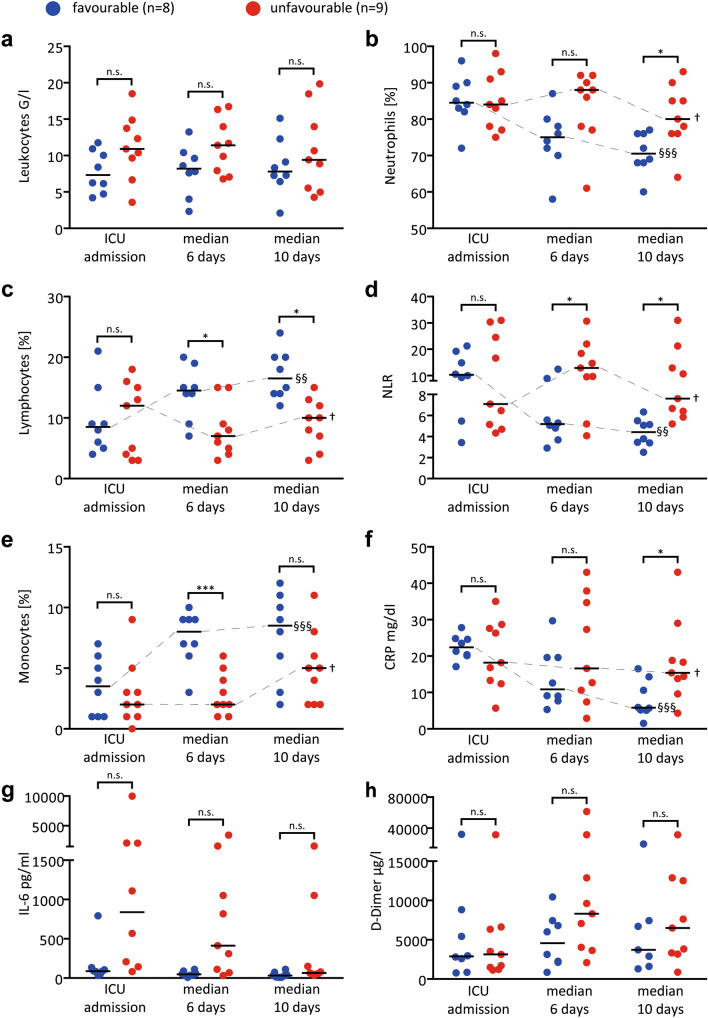
Severe COVID-19 associated respiratory failure, poses the one challenge of our days. Assessment and treatment of COVID-19 associated hyperinflammation may be key to improve outcomes. It was speculated that in subgroups of patients secondary hemophagocytic lymphohistiocytosis (sHLH) or cytokine release syndrome (CRS) with features of macrophage activation syndrome might drive severe disease trajectories. If confirmed, profound immunosuppressive therapy would be a rationale treatment approach. Over a median observation period of 11 (IQR: 8; 16) days, 19 consecutive confirmed severe COVID-19-patients admitted to our intensive-care-unit were tested for presence of sHLH by two independent experts. HScores and 2004-HLH diagnostic criteria were assessed. Patients were grouped according to short-term clinical courses: discharge from ICU versus ongoing ARDS or death at time of analysis. The median HScore at admission was 157 (IQR: 98;180), without the key clinical triad of HLH, i.e. progressive cytopenia, persistent fever and organomegaly. Independent expert chart review revealed the absence of sHLH in all cases. No patient reached more than 3/6 of modified HLH 2004 criteria. Nevertheless, patients presented hyperinflammation with peripheral neutrophilic signatures (neutrophil/lymphocyte-ratio > 3.5). The latter best paralleled their short-term clinical courses, with declining relative neutrophil numbers prior to extubation (4.4, [IQR: 2.5;6.3]; n = 8) versus those with unfavourable courses (7.6, [IQR: 5.2;31], n = 9). Our study rules out virus induced sHLH as the leading cause of most severe-COVID-19 trajectories. Instead, an associated innate neutrophilic hyperinflammatory response or virus-associated-CRS appears dominant in patients with an unfavourable clinical course. Therapeutic implications are discussed.
Conflict of interest statement
Dr. LaRosée reports personal fees from SOBI, personal fees and other from Novartis, outside the submitted work, none of the other authors has conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
