

Disentangling etiologies of CNS infections in Singapore using multiple correspondence analysis and random forest
- PMID: 33106525
- PMCID: PMC7588471
- DOI: 10.1038/s41598-020-75088-4
Disentangling etiologies of CNS infections in Singapore using multiple correspondence analysis and random forest
Abstract
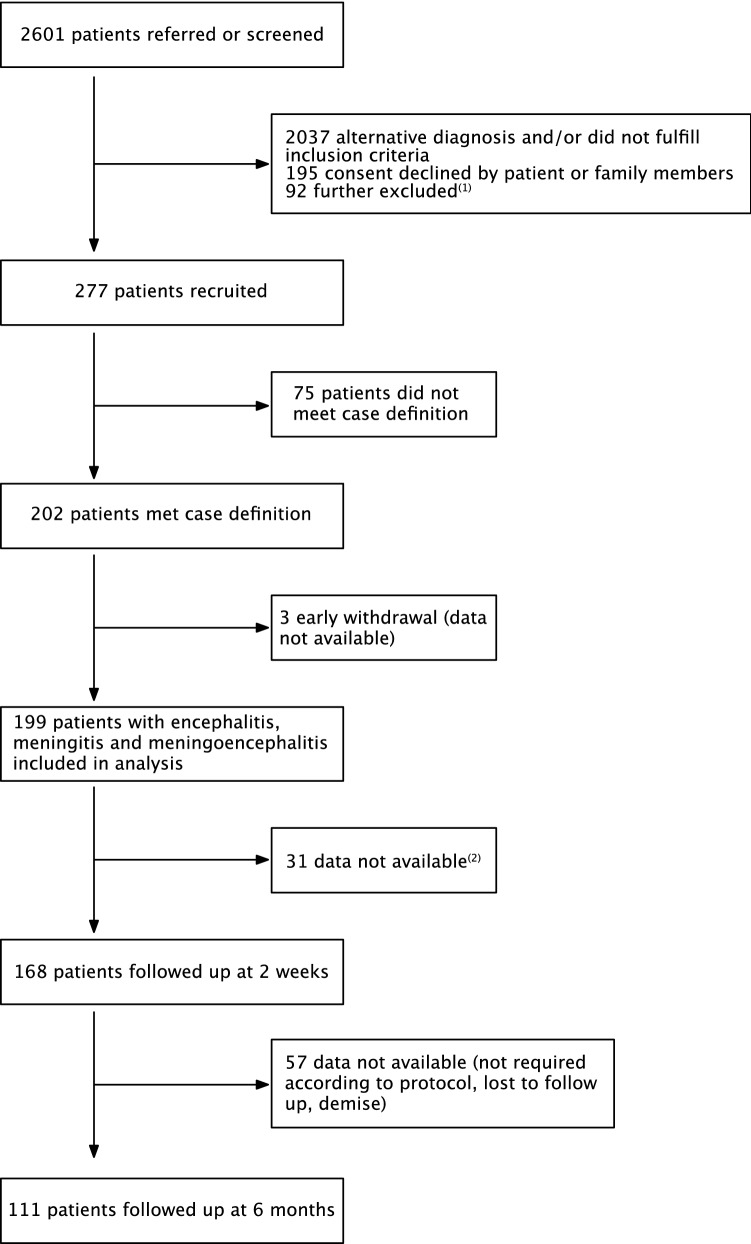
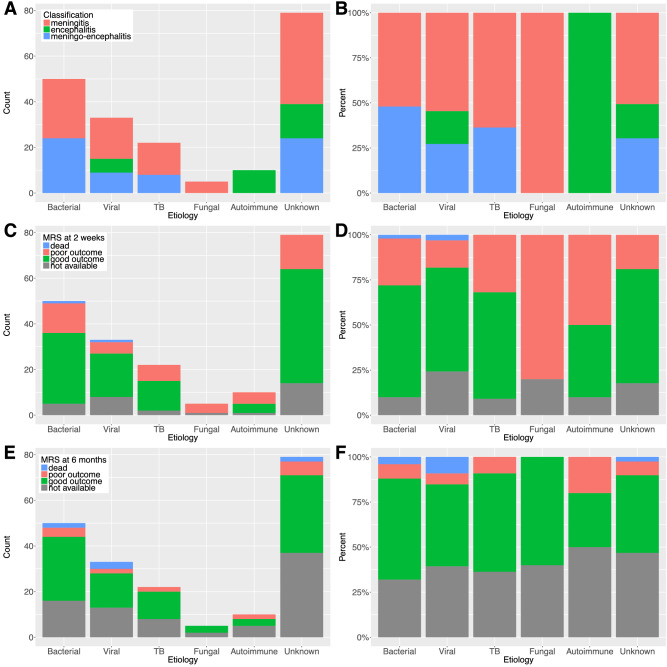
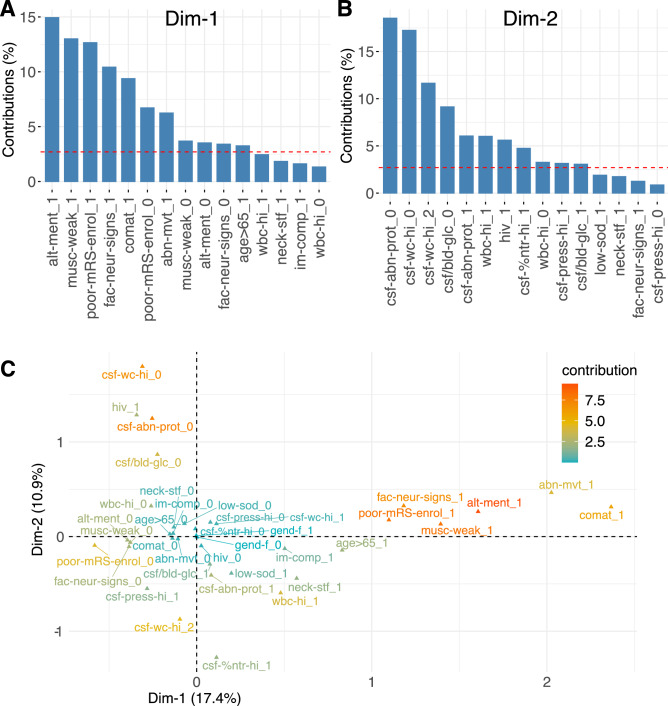
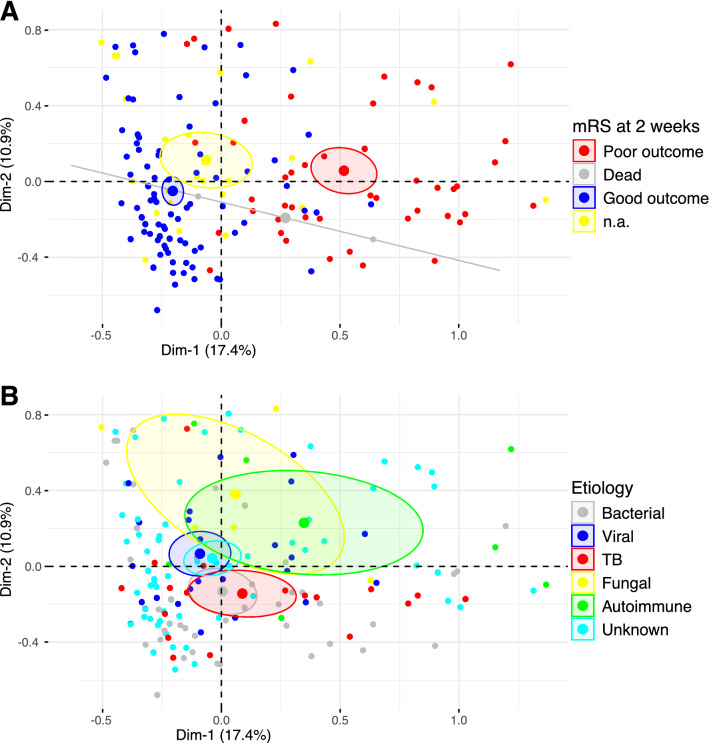
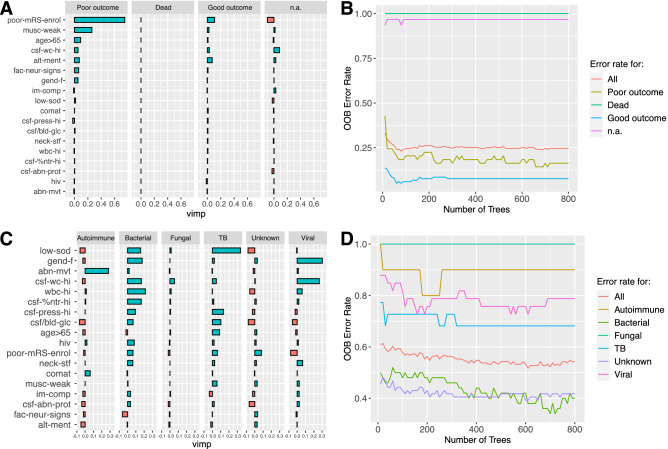
Central nervous system (CNS) infections cause substantial morbidity and mortality worldwide, with mounting concern about new and emerging neurologic infections. Stratifying etiologies based on initial clinical and laboratory data would facilitate etiology-based treatment rather than relying on empirical treatment. Here, we report the epidemiology and clinical outcomes of patients with CNS infections from a prospective surveillance study that took place between 2013 and 2016 in Singapore. Using multiple correspondence analysis and random forest, we analyzed the link between clinical presentation, laboratory results, outcome and etiology. Of 199 patients, etiology was identified as infectious in 110 (55.3%, 95%-CI 48.3-62.0), immune-mediated in 10 (5.0%, 95%-CI 2.8-9.0), and unknown in 79 patients (39.7%, 95%-CI 33.2-46.6). The initial presenting clinical features were associated with the prognosis at 2 weeks, while laboratory-related parameters were related to the etiology of CNS disease. The parameters measured were helpful to stratify etiologies in broad categories, but were not able to discriminate completely between all the etiologies. Our results suggest that while prognosis of CNS is clearly related to the initial clinical presentation, pinpointing etiology remains challenging. Bio-computational methods which identify patterns in complex datasets may help to supplement CNS infection diagnostic and prognostic decisions.
Conflict of interest statement
K.T. has received travel grants and compensation from Novartis, Merck, Sanofi, Eisai and Viela Bio for consulting services. The University of Oxford and A.V. hold patents for MuSK, LGI1 and CASPR2 antibody assays, licensed to Athena Diagnostics and Euroimmun AG. A.V. receives a proportion of royalties. All other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
