

Improving Blood Pressure Management in Primary Care Patients with Chronic Kidney Disease: a Systematic Review of Interventions and Implementation Strategies
- PMID: 33107008
- PMCID: PMC7652970
- DOI: 10.1007/s11606-020-06103-7
Improving Blood Pressure Management in Primary Care Patients with Chronic Kidney Disease: a Systematic Review of Interventions and Implementation Strategies
Abstract
Introduction: Chronic kidney disease (CKD) is widely prevalent, associated with morbidity and mortality, but may be lessened with timely implementation of evidence-based strategies including blood pressure (BP) control. Nonetheless, an evidence-practice gap persists. We synthesize the evidence for clinician-facing interventions to improve hypertension management in CKD patients in primary care.
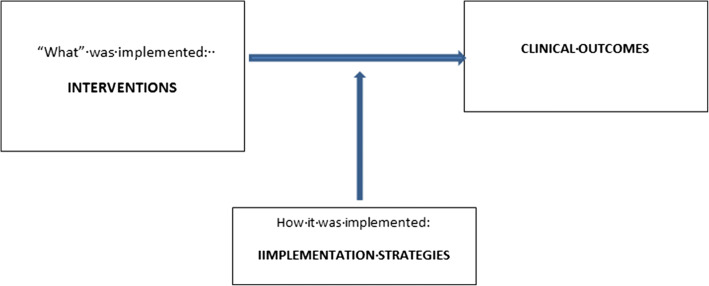
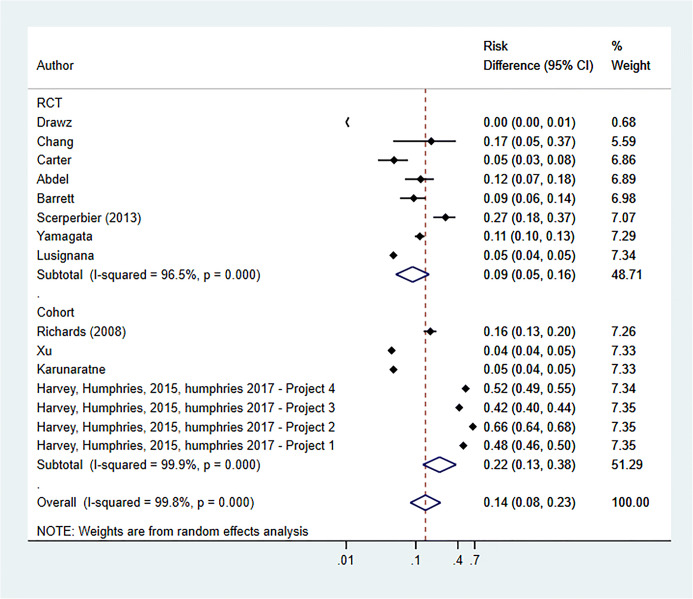
Methods: Electronic databases and related publications were queried for relevant studies. We used a conceptual model to address heterogeneity of interventions. We conducted a quantitative synthesis of interventions on blood pressure (BP) outcomes and a narrative synthesis of other CKD relevant clinical outcomes. Planned subgroup analyses were performed by (1) study design (randomized controlled trials (RCTs) or nonrandomized studies (NRS)); (2) intervention type (guideline-concordant decision support, shared care, pharmacist-facing); and (3) use of behavioral/implementation theory.
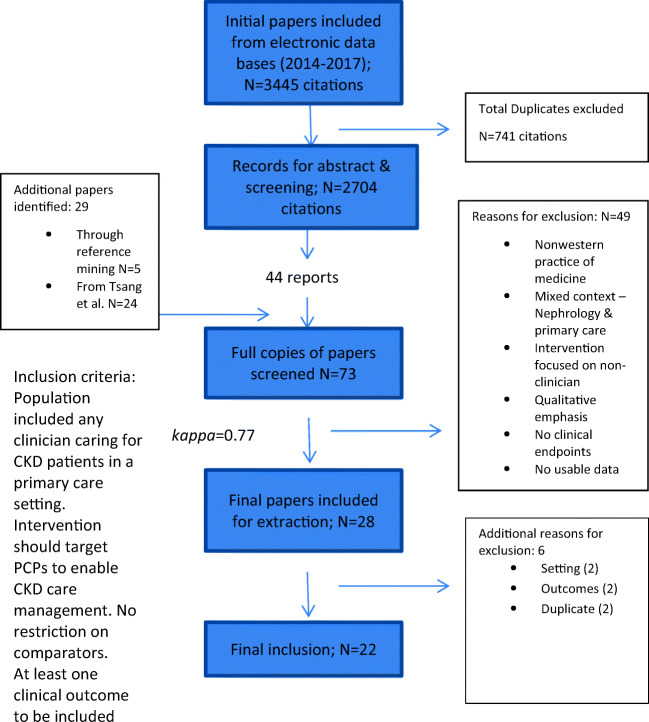
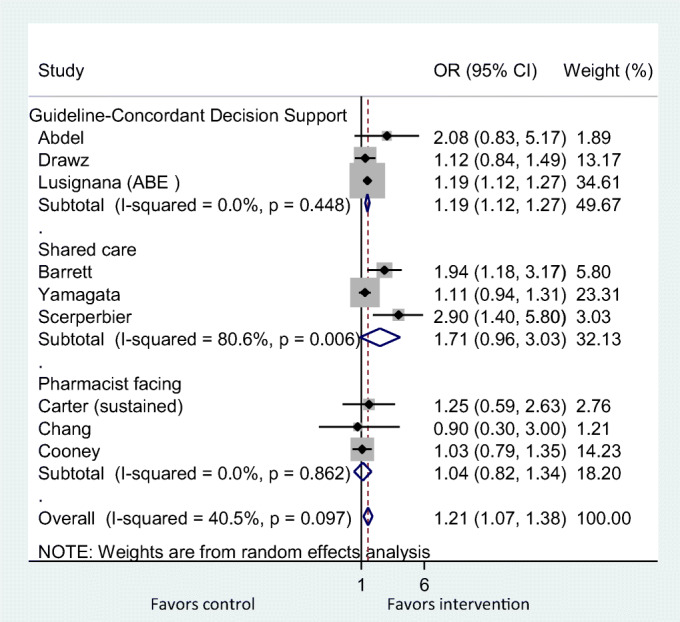
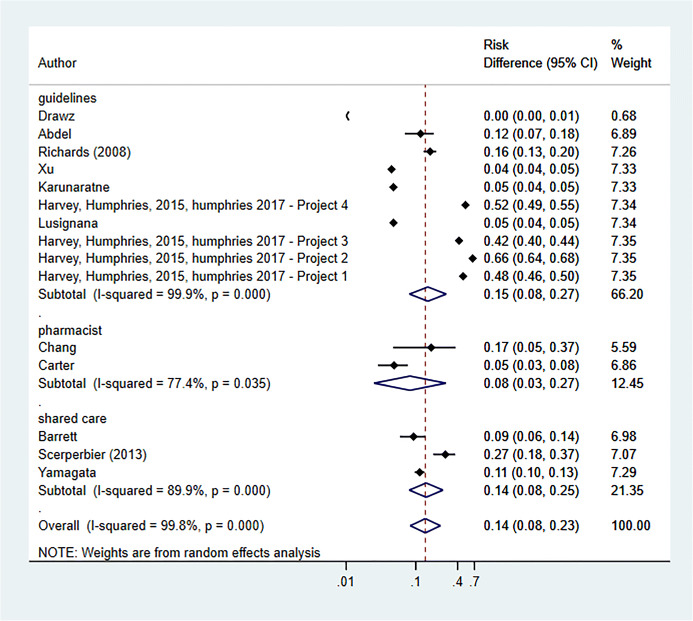
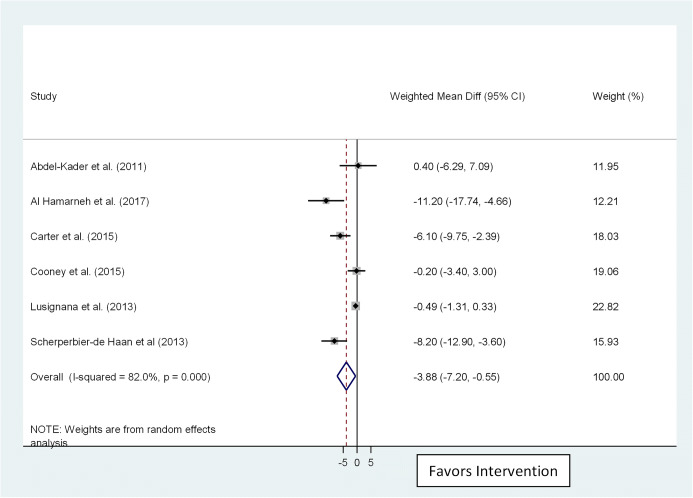
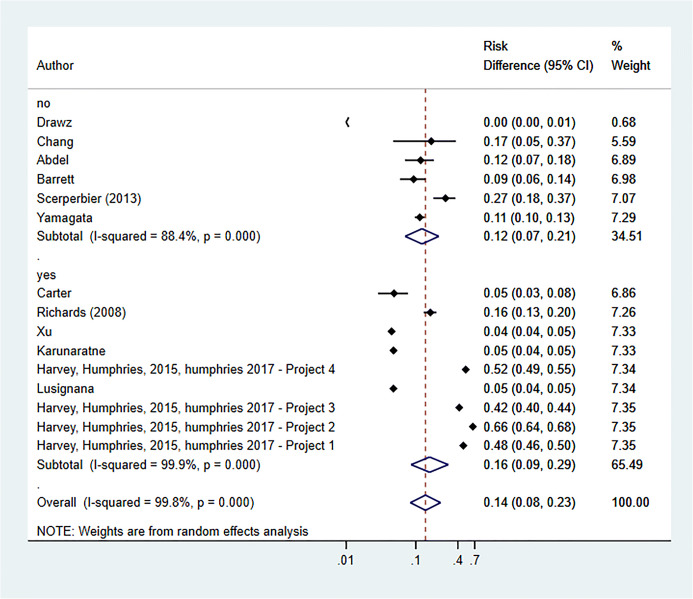
Results: Of 2704 manuscripts screened, 73 underwent full-text review; 22 met inclusion criteria. BP target achievement was reported in 15 and systolic BP reduction in 6 studies. Among RCTs, all interventions had a significant effect on BP control, (pooled OR 1.21; 95% CI 1.07 to 1.38). Subgroup analysis by intervention type showed significant effects for guideline-concordant decision support (pooled OR 1.19; 95% CI 1.12 to 1.27) but not shared care (pooled OR 1.71; 95% CI 0.96 to 3.03) or pharmacist-facing interventions (pooled OR 1.04; 95% CI 0.82 to 1.34). Subgroup analysis finding was replicated with pooling of RCTs and NRS. The five contributing studies showed large and significant reduction in systolic BP (pooled WMD - 3.86; 95% CI - 7.2 to - 0.55). Use of a behavioral/implementation theory had no impact, while RCTs showed smaller effect sizes than NRS.
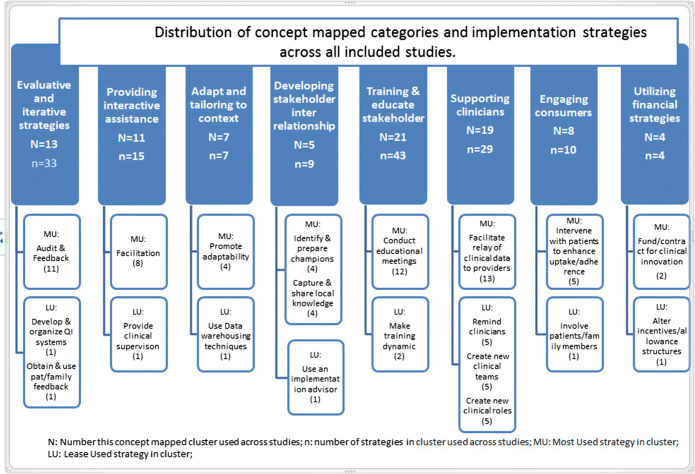
Discussion: Process-oriented implementation strategies used with guideline-concordant decision support was a promising implementation approach. Better reporting guidelines on implementation would enable more useful synthesis of the efficacy of CKD clinical interventions integrated into primary care.
Prospero registration number: CRD42018102441.
Keywords: blood pressure control; chronic kidney disease; guideline implementation; implementation strategies; primary care practitioner interventions; systematic review.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. Lancet. 2017;389(10075):1238–52. - PubMed
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–47. - PubMed
-
- Jha V, Garcia-Garcia G, Iseki K, Li Z, Naicker S, Plattner B, et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013;382(9888):260–72. - PubMed
-
- Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet. 2003;362(9391):1225–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
