

The expanding role of SGLT2 inhibitors beyond glucose-lowering to cardiorenal protection
- PMID: 33107349
- PMCID: PMC8592607
- DOI: 10.1080/07853890.2020.1841281
The expanding role of SGLT2 inhibitors beyond glucose-lowering to cardiorenal protection
Abstract
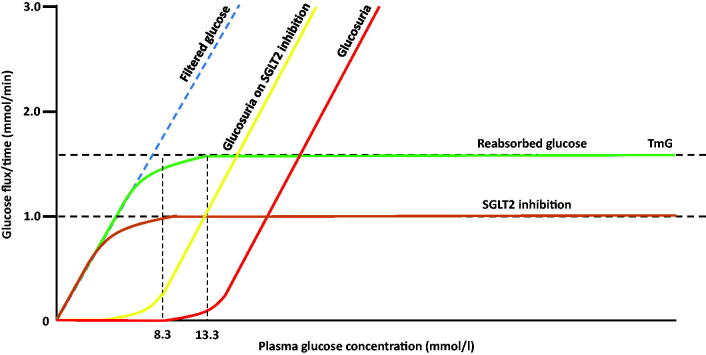
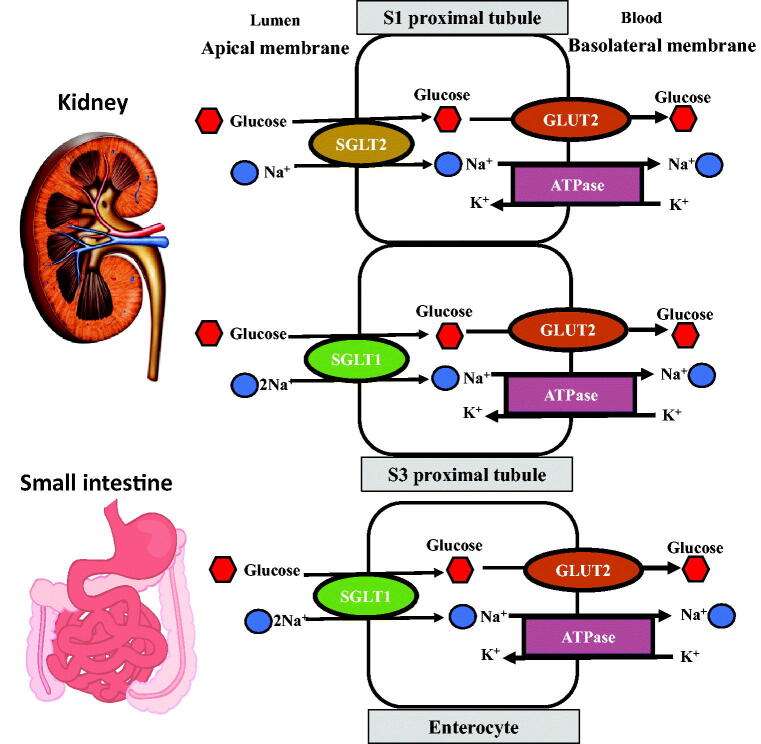
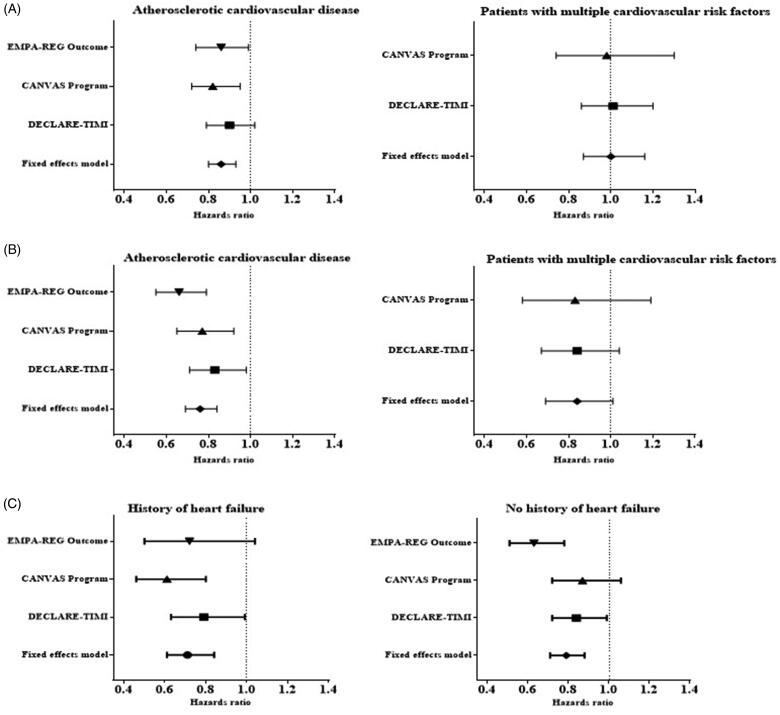
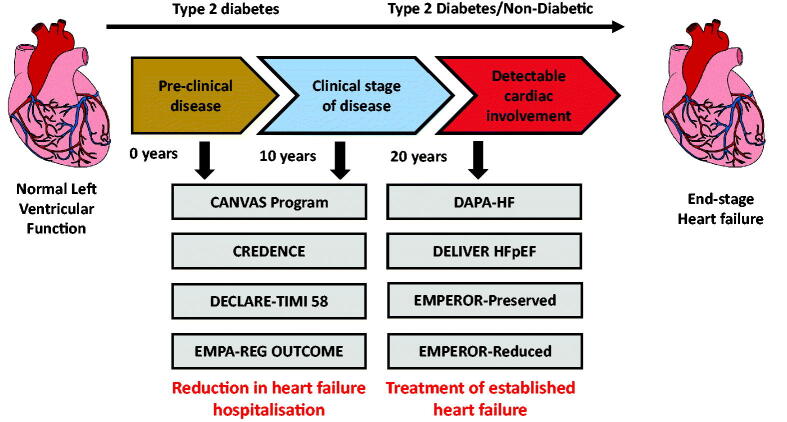
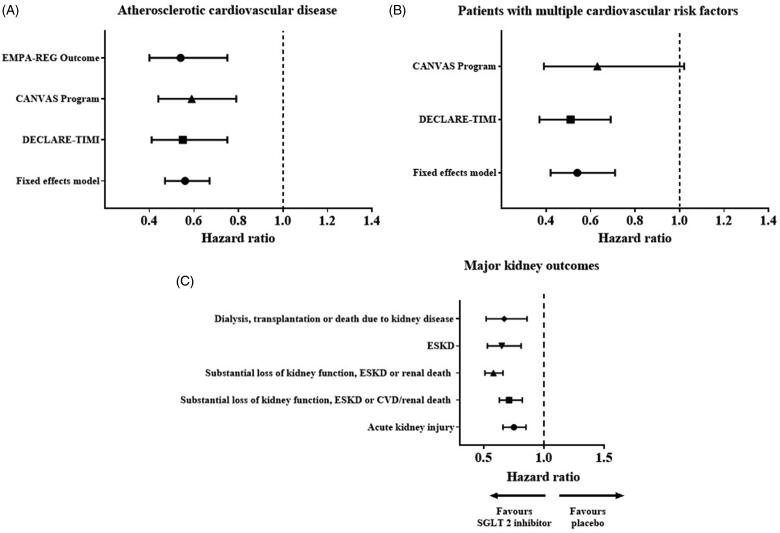
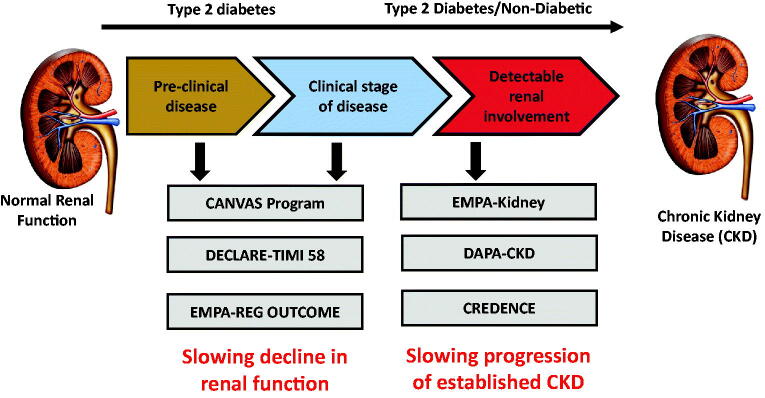
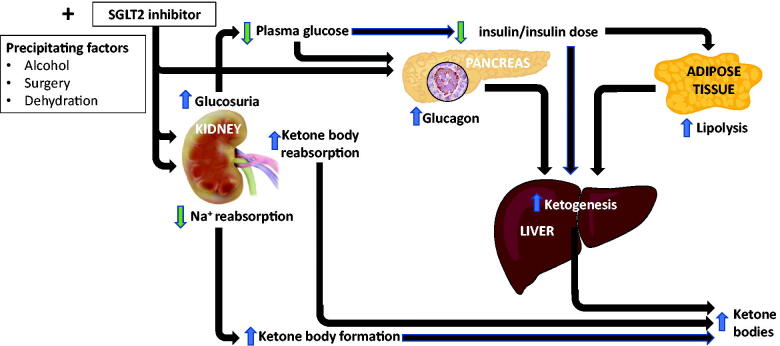
The kidney plays a major physiological role in glucose homeostasis but also contributes to the pathophysiology of type 2 diabetes (T2D), mediated by renal sodium glucose cotransporters (SGLTs). This recognition led to the development of SGLT2 inhibitors that inhibit proximal renal tubular renal glucose and sodium reabsorption. The glucoretic and natriuretic effect of SGLT2 inhibitors is associated with reductions in HbA1c levels, body weight, systolic blood pressure and triglycerides. Major vascular complications of T2D include cardiovascular disease and chronic kidney disease (CKD). Results from several cardiovascular outcome trials (CVOTs) with these drugs have highlighted benefits in reducing major adverse cardiovascular events by 11%, reducing the risk of cardiovascular death or hospitalization for heart failure (HF) by 23% and reducing the risk of progression of renal disease by 45%. Their cardiorenal benefits are apparent across a range of eGFRs (within CKD1-3 groups) and the presence or absence of ischaemic heart disease, HF or T2D. In patients with HF with reduced ejection fraction (HFrEF), similar risk reductions in cardiovascular death and HF events are also seen; results from studies in patients with HF with preserved ejection fraction (HFpEF) are awaited. Cardiorenal benefits have been recently reported in patients with CKD, regardless of the presence or absence of T2D. Indications for use of SGLT2 inhibitors have extended beyond glucose-lowering to a central role in cardiorenal protection. This review will first explore the mechanisms by which glycaemic control, weight loss and cardiovascular risk factors are modulated therapeutically with SGLT2 inhibitors. Subsequently, we outline putative mechanisms underpinning the cardiorenal benefits seen, including in HF and CKD, in the context of completed and ongoing clinical studies. Treatment strategies with SGLT2 inhibitors in individuals with CKD or HF, with and/or without T2D are increasingly appealing. Combination therapy with complementary therapeutic agents is also explored.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Bergman H, Drury DR.. The relationship of kidney function to the glucose utilization of the extra abdominal tissues. Am J Physiol. 1938;124(2):279–284.
-
- Mather A, Pollock C.. Glucose handling by the kidney. Kidney Int. 2011;79:S1–S6. - PubMed
-
- Rahmoune H, Thompson PW, Ward JM, et al. . Glucose transporters in human renal proximal tubular cells isolated from the urine of patients with non-insulin-dependent diabetes. Diabetes. 2005;54(12):3427–3434. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous