Effect of Catheter Ablation With Vein of Marshall Ethanol Infusion vs Catheter Ablation Alone on Persistent Atrial Fibrillation: The VENUS Randomized Clinical Trial
- PMID: 33107945
- PMCID: PMC7592031
- DOI: 10.1001/jama.2020.16195
Effect of Catheter Ablation With Vein of Marshall Ethanol Infusion vs Catheter Ablation Alone on Persistent Atrial Fibrillation: The VENUS Randomized Clinical Trial
Abstract
Importance: Catheter ablation of persistent atrial fibrillation (AF) has limited success. Procedural strategies beyond pulmonary vein isolation have failed to consistently improve results. The vein of Marshall contains innervation and AF triggers that can be ablated by retrograde ethanol infusion.
Objective: To determine whether vein of Marshall ethanol infusion could improve ablation results in persistent AF when added to catheter ablation.
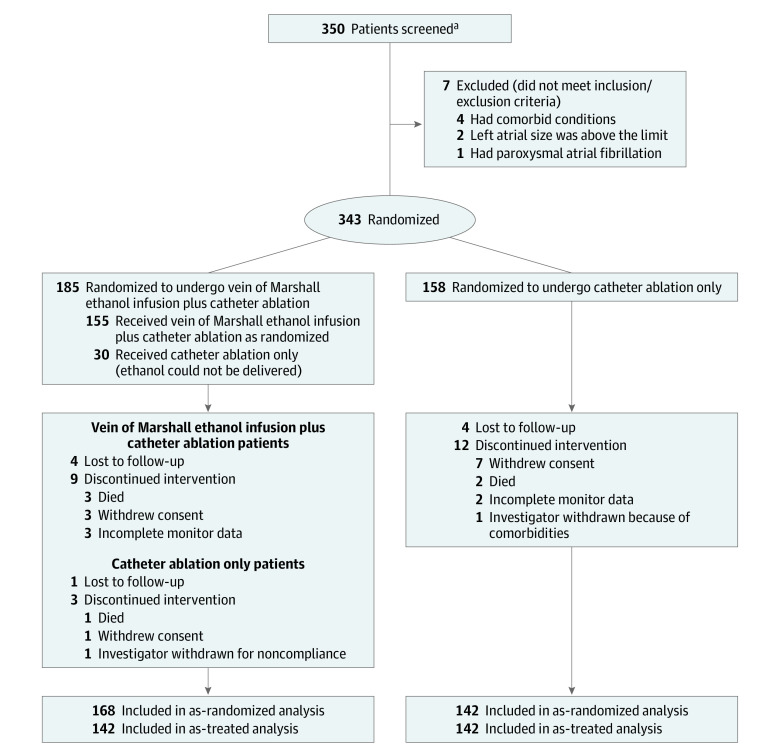
Design, setting, and participants: The Vein of Marshall Ethanol for Untreated Persistent AF (VENUS) trial was an investigator-initiated, National Institutes of Health-funded, randomized, single-blinded trial conducted in 12 centers in the United States. Patients (N = 350) with persistent AF referred for first ablation were enrolled from October 2013 through June 2018. Follow-up concluded in June 2019.
Interventions: Patients were randomly assigned to catheter ablation alone (n = 158) or catheter ablation combined with vein of Marshall ethanol infusion (n = 185) in a 1:1.15 ratio to accommodate for 15% technical vein of Marshall ethanol infusion failures.
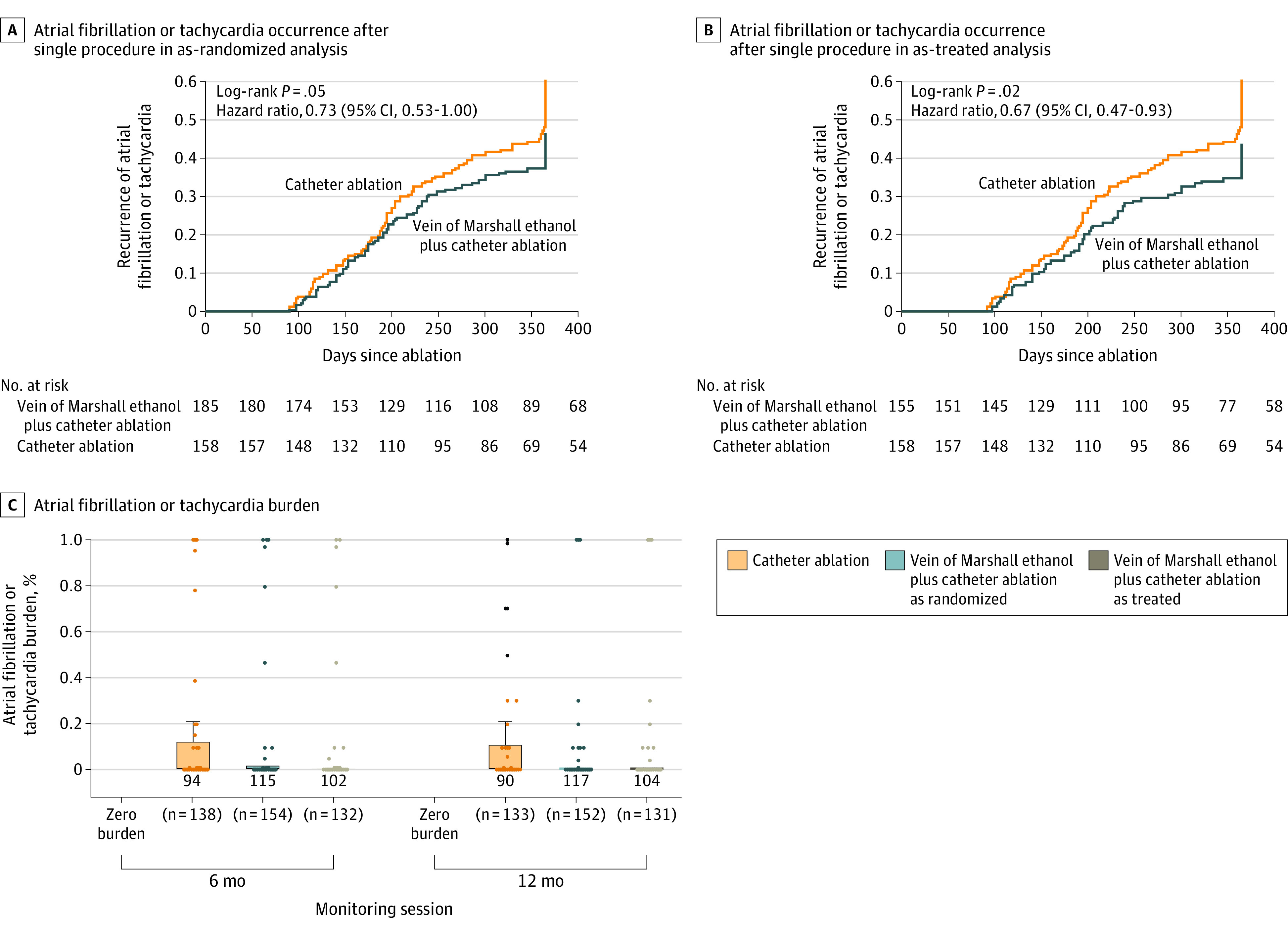
Main outcomes and measures: The primary outcome was freedom from AF or atrial tachycardia for longer than 30 seconds after a single procedure, without antiarrhythmic drugs, at both 6 and 12 months. Outcome assessment was blinded to randomization treatment. There were 12 secondary outcomes, including AF burden, freedom from AF after multiple procedures, perimitral block, and others.
Results: Of the 343 randomized patients (mean [SD] age, 66.5 [9.7] years; 261 men), 316 (92.1%) completed the trial. Vein of Marshall ethanol was successfully delivered in 155 of 185 patients. At 6 and 12 months, the proportion of patients with freedom from AF/atrial tachycardia after a single procedure was 49.2% (91/185) in the catheter ablation combined with vein of Marshall ethanol infusion group compared with 38% (60/158) in the catheter ablation alone group (difference, 11.2% [95% CI, 0.8%-21.7%]; P = .04). Of the 12 secondary outcomes, 9 were not significantly different, but AF burden (zero burden in 78.3% vs 67.9%; difference, 10.4% [95% CI, 2.9%-17.9%]; P = .01), freedom from AF after multiple procedures (65.2% vs 53.8%; difference, 11.4% [95% CI, 0.6%-22.2%]; P = .04), and success achieving perimitral block (80.6% vs 51.3%; difference, 29.3% [95% CI, 19.3%-39.3%]; P < .001) were significantly improved in vein of Marshall-treated patients. Adverse events were similar between groups.
Conclusions and relevance: Among patients with persistent AF, addition of vein of Marshall ethanol infusion to catheter ablation, compared with catheter ablation alone, increased the likelihood of remaining free of AF or atrial tachycardia at 6 and 12 months. Further research is needed to assess longer-term efficacy.
Trial registration: ClinicalTrials.gov Identifier: NCT01898221.
Conflict of interest statement
Figures