

Hybrid technique of virtual-assisted lung mapping and systemic indocyanine green injection for extended segmentectomy
- PMID: 33108570
- PMCID: PMC7591651
- DOI: 10.1186/s40792-020-01052-z
Hybrid technique of virtual-assisted lung mapping and systemic indocyanine green injection for extended segmentectomy
Abstract
Background: Various approaches have been used to assist and facilitate segmentectomy with favorable oncological outcomes. We describe a hybrid approach comprising virtual-assisted lung mapping (VAL-MAP), which is a preoperative bronchoscopic dye-marking technique, combined with systemic indocyanine green (ICG) injection.
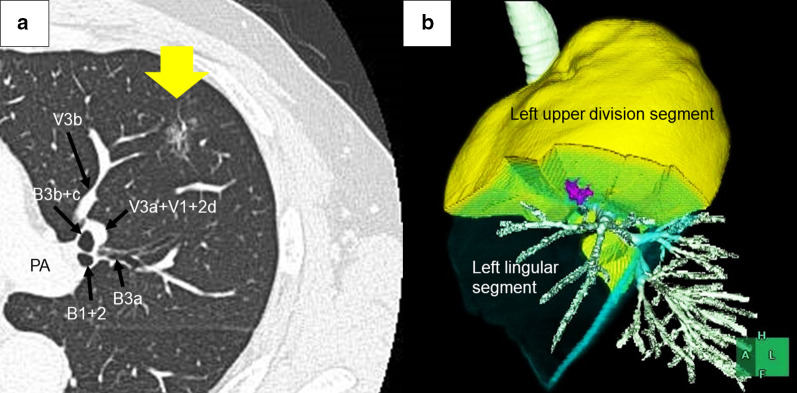
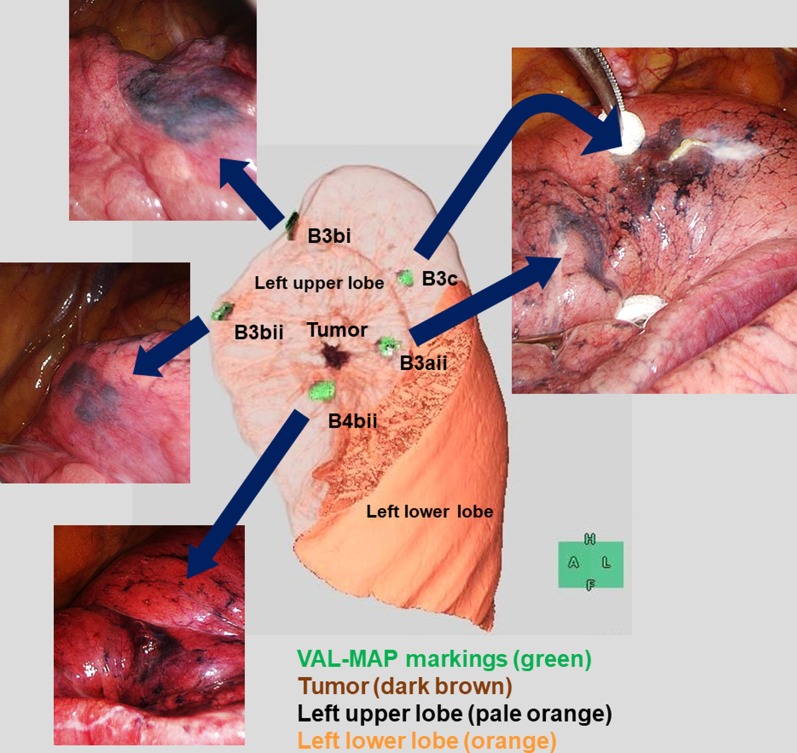
Clinical presentation: An asymptomatic 64-year-old man was referred to our department because of a lung nodule detected during his annual medical checkup. The chest computed-tomography image revealed a 16-mm, partly solid, ground-glass nodule in the left segment 4. Because the nodule was hardly palpable and deeply located between the left upper division segment and the left lingular segment, we performed VAL-MAP to facilitate extended left lingulectomy. Five dye markings were undertaken preoperatively. Surgery to remove the nodule was then conducted via complete three-port video-assisted thoracic surgery. The VAL-MAP markings were easily identified intraoperatively and helped locate the nodule. The intersegmental plane was identified by the ICG injection. The resection line was determined based on the intersegmental plane identified by the ICG injection and the site of the nodule suggested by the VAL-MAP markings. Following the resection line, we thoracoscopically achieved extended lingulectomy with sufficient surgical margins. The patient was discharged with no complications. The pathological diagnosis was adenocarcinoma in situ.
Conclusion: The hybrid technique of VAL-MAP and systemic ICG injection can be useful for accomplishing successful extended segmentectomy.
Keywords: Bronchoscopy; Indocyanine green; Intersegmental plane; Lung cancer; Segmentectomy; Thoracic surgery; Video-assisted thoracic surgery; Virtual-assisted lung mapping.
Conflict of interest statement
The authors declare no conflict of interest related to this study.
Figures


References
LinkOut - more resources
Full Text Sources
