

Concurrent hiatal hernia repair and bariatric surgery: outcomes after sleeve gastrectomy and Roux-en-Y gastric bypass
- PMID: 33109444
- PMCID: PMC8116048
- DOI: 10.1016/j.soard.2020.08.035
Concurrent hiatal hernia repair and bariatric surgery: outcomes after sleeve gastrectomy and Roux-en-Y gastric bypass
Abstract
Background: Hiatal hernias are often repaired concurrently with bariatric surgery to reduce risk of gastroesophageal reflux disease-related complications.
Objectives: To examine the association between concurrent hiatal hernia repair (HHR) and bariatric outcomes.
Setting: A 2010-2017 U.S. commercial insurance claims data set.
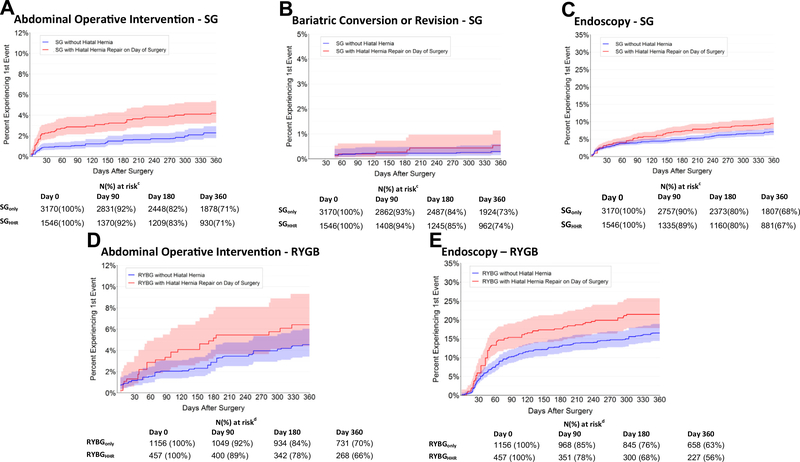
Methods: We conducted a retrospective cohort study. We identified adults who underwent sleeve gastrectomy (SG) or Roux-en-Y gastric bypass (RYGB) alone or had bariatric surgery concurrently with HHR. We matched patients with and without HHR and followed patients up to 3 years for incident abdominal operative interventions, bariatric revisions/conversions, and endoscopy. Time to first event for each outcome was compared using multivariable Cox proportional hazards modeling.
Results: We matched 1546 SG patients with HHR to 3170 SG patients without HHR, and we matched 457 RYGB patients with HHR to 1156 RYGB patients without HHR. A total of 73% had a full year of postoperative enrollment. Patients who underwent concurrent SG and HHR were more likely to have additional abdominal operations (adjusted hazard ratio [aHR], 2.1; 95% CI, 1.5-3.1) and endoscopies (aHR, 1.5; 95% CI, 1.2-1.8) but not bariatric revisions/conversions (aHR, 1.7; 95% CI, .6-4.6) by 1 year after surgery, a pattern maintained at 3 years of follow-up. Among RYGB patients, concurrent HHR was associated only with an increased risk of endoscopy (aHR, 1.4; 95% CI, 1.1-1.8)) at 1 year of follow-up, persisting at 3 years.
Conclusions: Concurrent SG/HHR was associated with increased risk of some subsequent operative and nonoperative interventions, a pattern that was not consistently observed for RYGB. Additional studies could examine whether changes to concurrent HHR technique could reduce risk.
Keywords: Gastric bypass; Hiatal hernia repair; Sleeve gastrectomy.
Copyright © 2020 American Society for Bariatric Surgery. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bakhos CT, Patel SP, Petrov RV, Abbas AES. Management of paraesophageal hernia in the morbidly obese patient. Thorac Surg Clin 2019;29(4):379–86. - PubMed
-
- Che F, Nguyen B, Cohen A, Nguyen NT. Prevalence of hiatal hernia in the morbidly obese. Surg Obes Relat Dis 2013;9(6):920–4. - PubMed
-
- Callaway JP, Vaezi MF. Hiatal and paraesophageal hernias. Clin Gastroenterol Hepatol 2018;16(6):810–3. - PubMed
-
- DuPree CE, Blair K, Steele SR, Martin MJ. Laparoscopic sleeve gastrectomy in patients with preexisting gastroesophageal reflux disease: a national analysis. JAMA Surg 2014;149(4):328–34. - PubMed
-
- Obeid T, Krishnan A, Abdalla G, Schweitzer M, Magnuson T, Steele KE. GERD is associated with higher long-term reoperation rates after bariatric surgery. J Gastrointest Surg 2016;20(1):119–24:discussion 124. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
