

Hospitalised COVID-19 patients of the Mount Sinai Health System: a retrospective observational study using the electronic medical records
- PMID: 33109676
- PMCID: PMC7592304
- DOI: 10.1136/bmjopen-2020-040441
Hospitalised COVID-19 patients of the Mount Sinai Health System: a retrospective observational study using the electronic medical records
Abstract
Objective: To assess association of clinical features on COVID-19 patient outcomes.
Design: Retrospective observational study using electronic medical record data.
Setting: Five member hospitals from the Mount Sinai Health System in New York City (NYC).
Participants: 28 336 patients tested for SARS-CoV-2 from 24 February 2020 to 15 April 2020, including 6158 laboratory-confirmed COVID-19 cases.
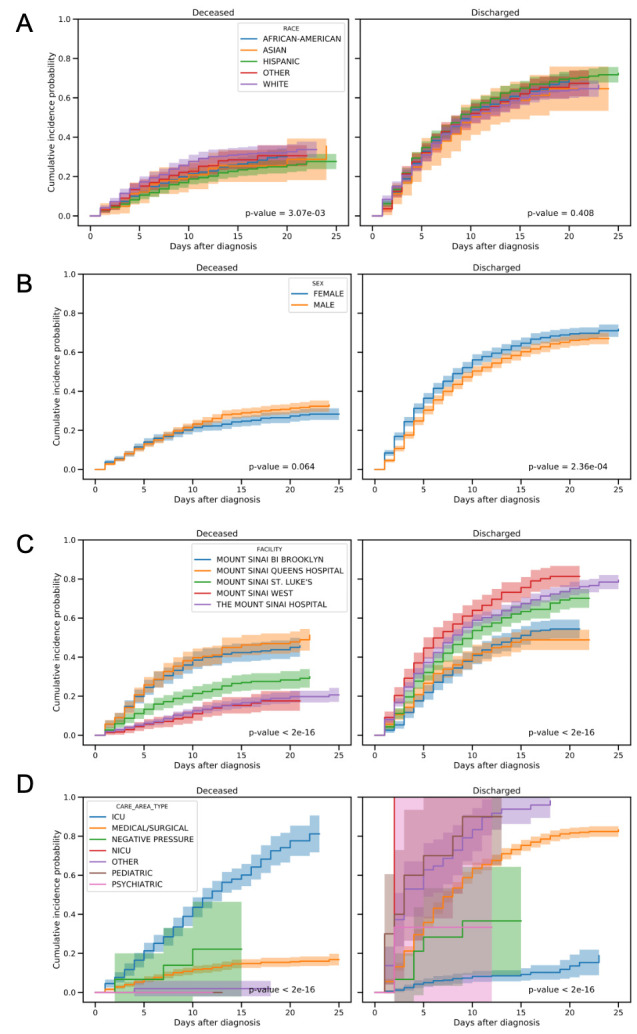
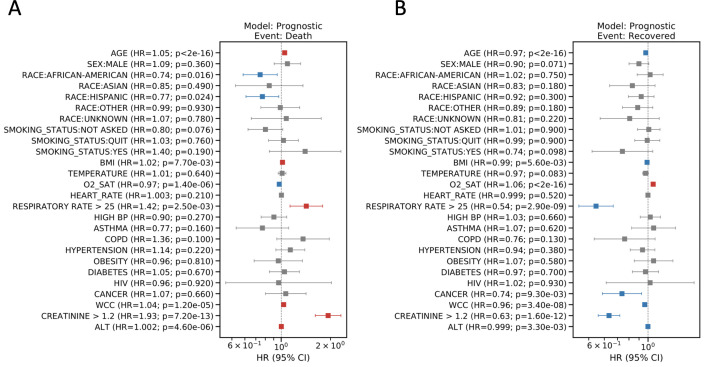
Main outcomes and measures: Positive test rates and in-hospital mortality were assessed for different racial groups. Among positive cases admitted to the hospital (N=3273), we estimated HR for both discharge and death across various explanatory variables, including patient demographics, hospital site and unit, smoking status, vital signs, lab results and comorbidities.
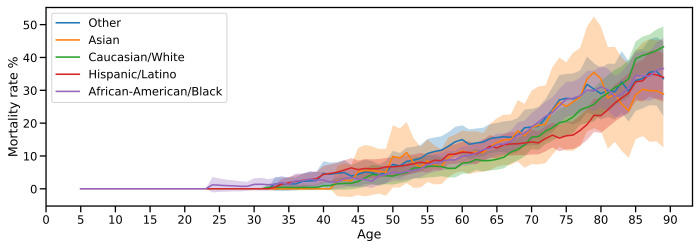
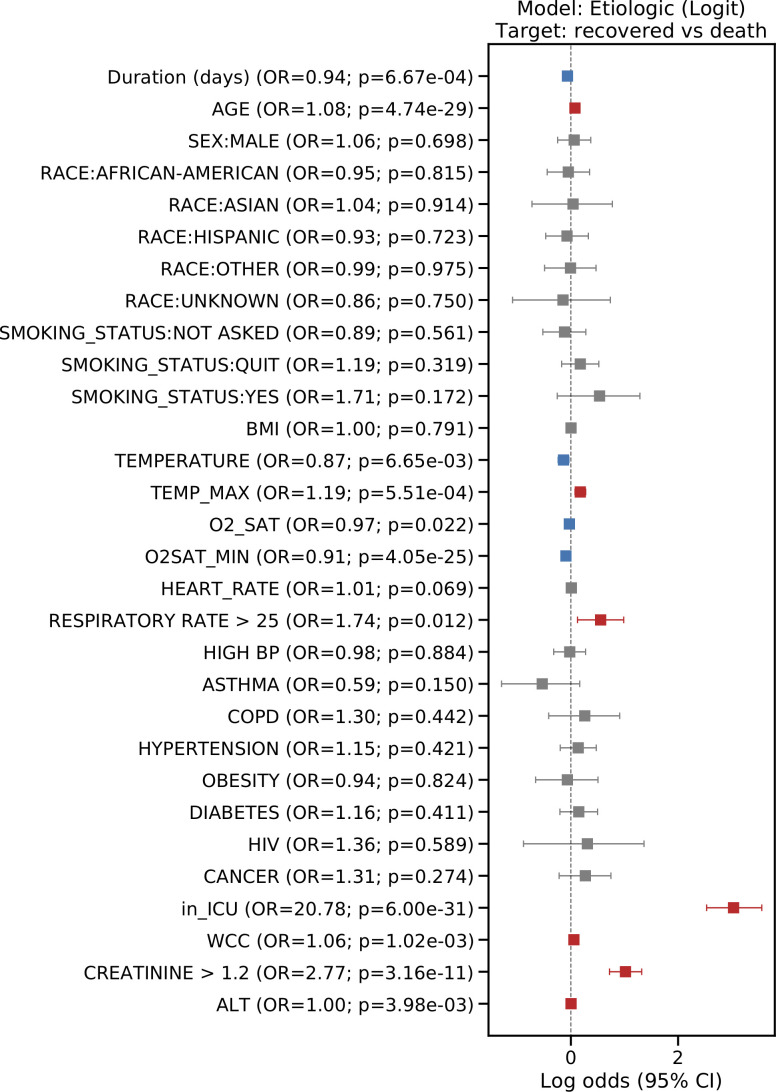
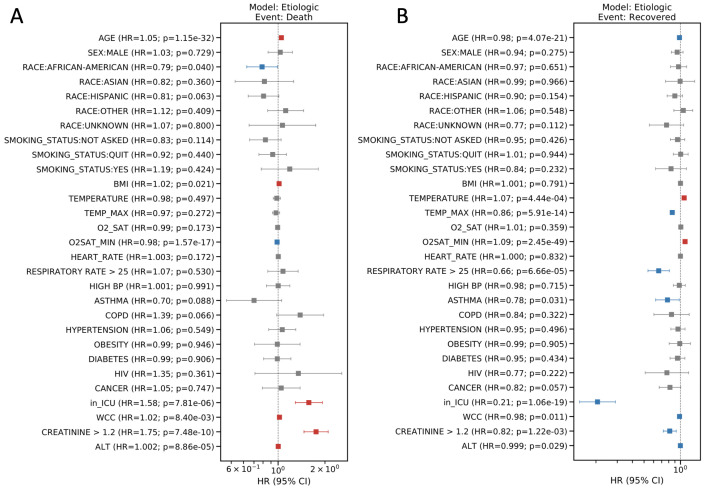
Results: Hispanics (29%) and African Americans (25%) had disproportionately high positive case rates relative to their representation in the overall NYC population (p<0.05); however, no differences in mortality rates were observed in hospitalised patients based on race. Outcomes differed significantly between hospitals (Gray's T=248.9; p<0.05), reflecting differences in average baseline age and underlying comorbidities. Significant risk factors for mortality included age (HR 1.05, 95% CI 1.04 to 1.06; p=1.15e-32), oxygen saturation (HR 0.985, 95% CI 0.982 to 0.988; p=1.57e-17), care in intensive care unit areas (HR 1.58, 95% CI 1.29 to 1.92; p=7.81e-6) and elevated creatinine (HR 1.75, 95% CI 1.47 to 2.10; p=7.48e-10), white cell count (HR 1.02, 95% CI 1.01 to 1.04; p=8.4e-3) and body mass index (BMI) (HR 1.02, 95% CI 1.00 to 1.03; p=1.09e-2). Deceased patients were more likely to have elevated markers of inflammation.
Conclusions: While race was associated with higher risk of infection, we did not find racial disparities in inpatient mortality suggesting that outcomes in a single tertiary care health system are comparable across races. In addition, we identified key clinical features associated with reduced mortality and discharge. These findings could help to identify which COVID-19 patients are at greatest risk of a severe infection response and predict survival.
Keywords: COVID-19; epidemiology; health informatics; infectious diseases.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: WKO is a paid consultant to Astellas, Astra Zeneca, Bayer, Janssen, Sanofi, Sema4, and TeneoBio.
Figures
References
-
- Tang W, Cao Z, Han M, et al. Hydroxychloroquine in patients with COVID-19: an open-label, randomized, controlled trial. medRxiv 2020.
-
- Health NDo Age adjusted rate of fatal lab confirmed COVID-19 cases per 100,000 by race/ethnicity group, 2020. Available: https://www1.nyc.gov/assets/doh/downloads/pdf/imm/covid-19-deaths-race-e...[Accessed 27 Jul 2020].
-
- Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospitalization and critical illness among 4103 patients with COVID-19 disease in New York City. medRxiv 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous