

Progress in the mechanism and targeted drug therapy for COPD
- PMID: 33110061
- PMCID: PMC7588592
- DOI: 10.1038/s41392-020-00345-x
Progress in the mechanism and targeted drug therapy for COPD
Abstract
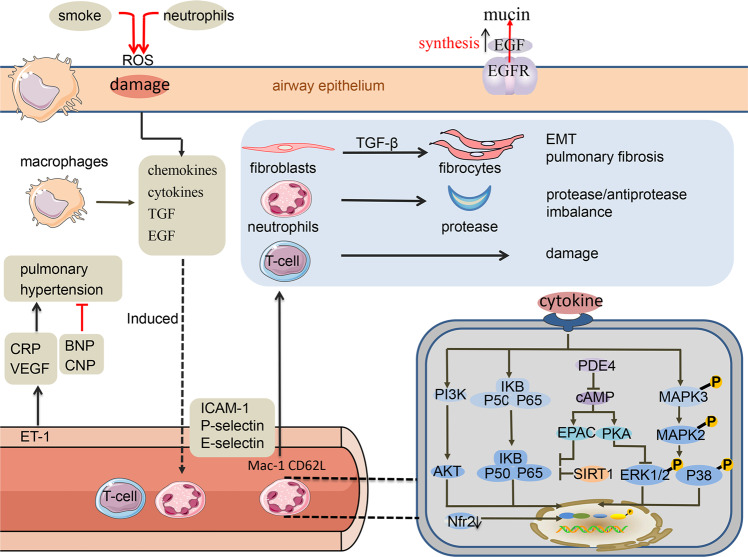
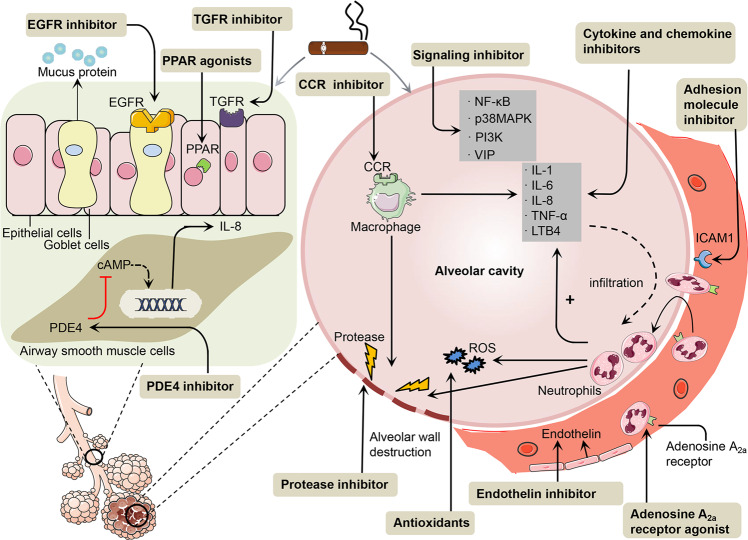
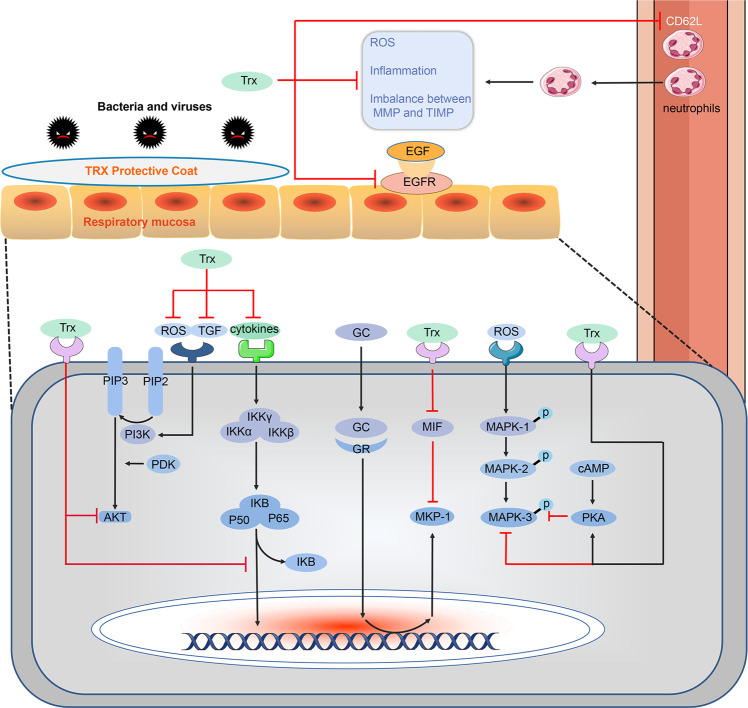
Chronic obstructive pulmonary disease (COPD) is emphysema and/or chronic bronchitis characterised by long-term breathing problems and poor airflow. The prevalence of COPD has increased over the last decade and the drugs most commonly used to treat it, such as glucocorticoids and bronchodilators, have significant therapeutic effects; however, they also cause side effects, including infection and immunosuppression. Here we reviewed the pathogenesis and progression of COPD and elaborated on the effects and mechanisms of newly developed molecular targeted COPD therapeutic drugs. Among these new drugs, we focussed on thioredoxin (Trx). Trx effectively prevents the progression of COPD by regulating redox status and protease/anti-protease balance, blocking the NF-κB and MAPK signalling pathways, suppressing the activation and migration of inflammatory cells and the production of cytokines, inhibiting the synthesis and the activation of adhesion factors and growth factors, and controlling the cAMP-PKA and PI3K/Akt signalling pathways. The mechanism by which Trx affects COPD is different from glucocorticoid-based mechanisms which regulate the inflammatory reaction in association with suppressing immune responses. In addition, Trx also improves the insensitivity of COPD to steroids by inhibiting the production and internalisation of macrophage migration inhibitory factor (MIF). Taken together, these findings suggest that Trx may be the ideal drug for treating COPD.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
