

Current NAFLD guidelines for risk stratification in diabetic patients have poor diagnostic discrimination
- PMID: 33110165
- PMCID: PMC7591877
- DOI: 10.1038/s41598-020-75227-x
Current NAFLD guidelines for risk stratification in diabetic patients have poor diagnostic discrimination
Abstract
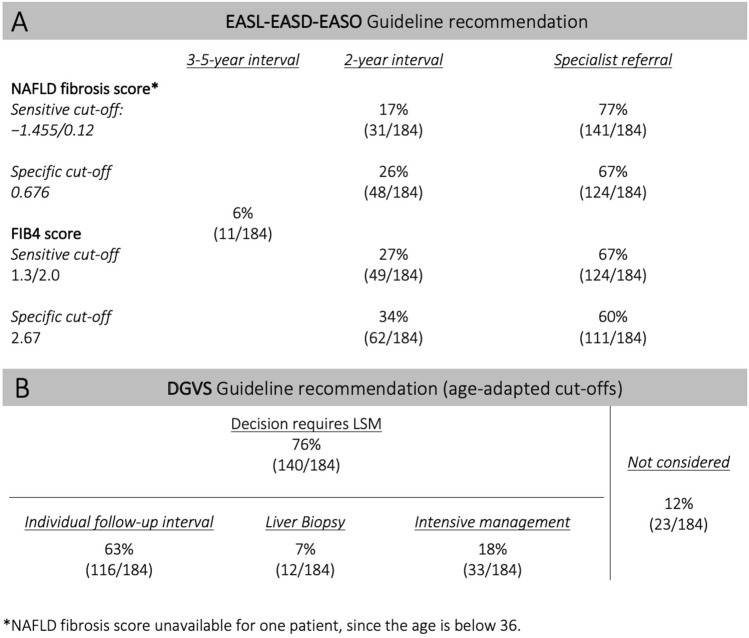
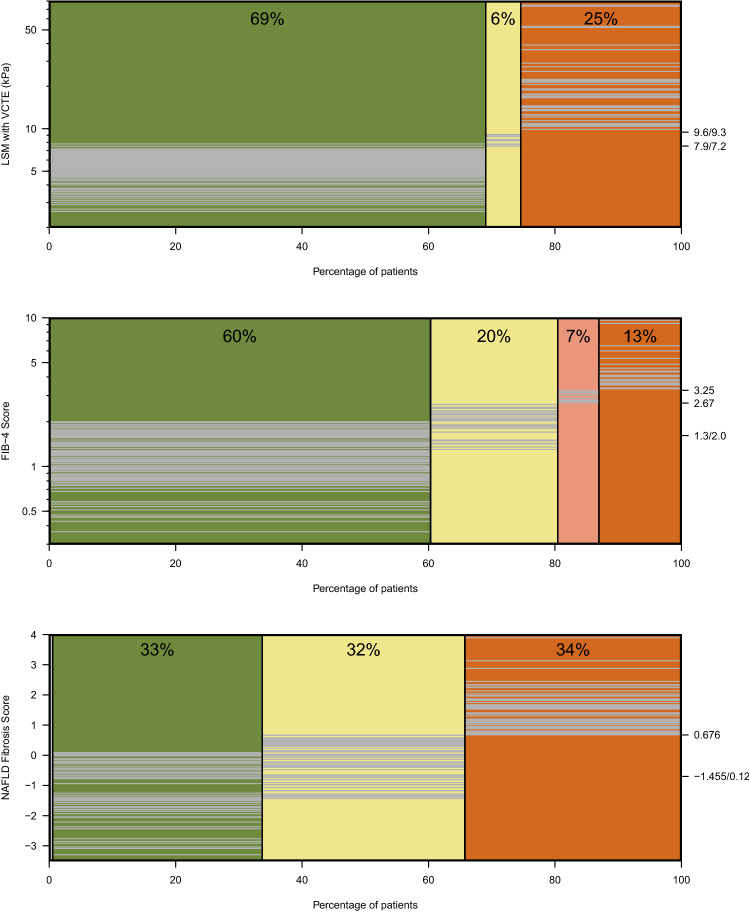
Patients with type 2 diabetes (T2D) are at risk for non-alcoholic fatty liver disease (NAFLD) and associated complications. This study evaluated the performance of international (EASL-EASD-EASO) and national (DGVS) guidelines for NAFLD risk stratification. Patients with T2D prospectively underwent ultrasound, liver stiffness measurement (LSM) and serum-based fibrosis markers. Guideline-based risk classification and referral rates for different screening approaches were compared and the diagnostic properties of simplified algorithms, genetic markers and a new NASH surrogate (FAST score) were evaluated. NAFLD risk was present in 184 of 204 screened patients (age 64.2 ± 10.7 years; BMI 32.6 ± 7.6 kg/m2). EASL-EASD-EASO recommended specialist referral for 60-77% depending on the fibrosis score used, only 6% were classified as low risk. The DGVS algorithm required LSM for 76%; 25% were referred for specialised care. The sensitivities of the diagnostic pathways were 47-96%. A simplified referral strategy revealed a sensitivity/specificity of 46/88% for fibrosis risk. Application of the FAST score reduced the referral rate to 35%. This study (a) underlines the high prevalence of fibrosis risk in T2D, (b) demonstrates very high referral rates for in-depth hepatological work-up, and (c) indicates that simpler referral algorithms may produce comparably good results and could facilitate NAFLD screening.
Conflict of interest statement
DP, TK and JW received an unrestricted research grant from Echosens, France. TK is an advisory board member for Echosens, France. Echosens provided the elastography device and performed FAST score calculation. SB, AB, MH (Maria Heni), TB, YB, AD, AT, MH, MB and VK does not have competing interest. We acknowledge support from the German Research Foundation (DFG) and Leipzig University within the program of Open Access Publishing. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Figures



References
-
- EASL, EASD & EASO. European Association For The Study Of The Liver (EASL) - European Association For The Study Of Diabetes (EASD) - European Association For The Study Of Obesity (EASO): Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Diabetologia59, 1121–1140 (2016). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
