

Best practices for the analytical validation of clinical whole-genome sequencing intended for the diagnosis of germline disease
- PMID: 33110627
- PMCID: PMC7585436
- DOI: 10.1038/s41525-020-00154-9
Best practices for the analytical validation of clinical whole-genome sequencing intended for the diagnosis of germline disease
Abstract
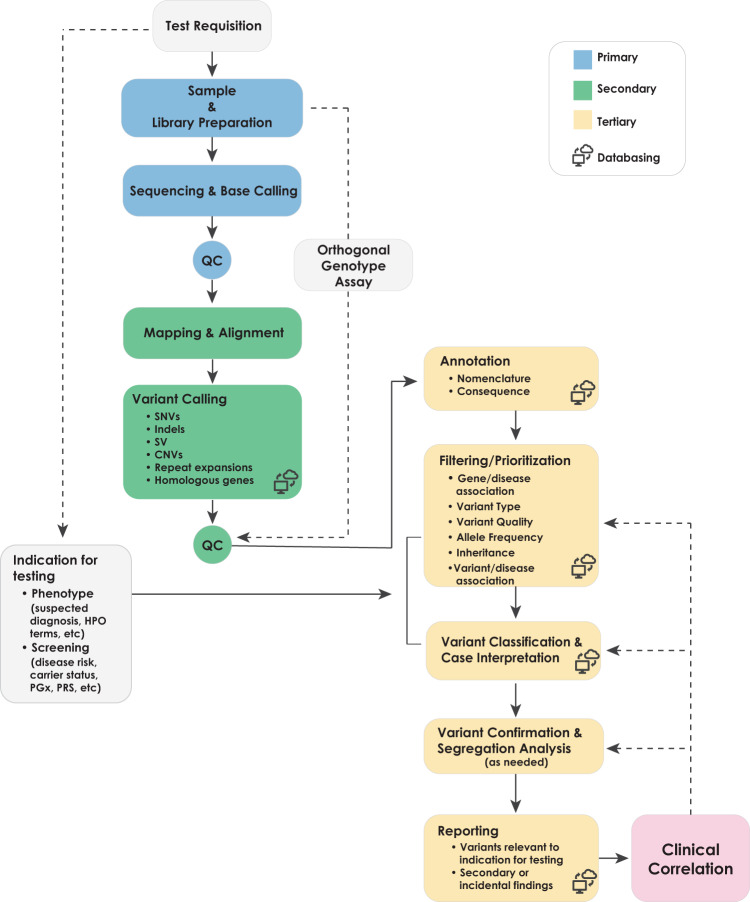
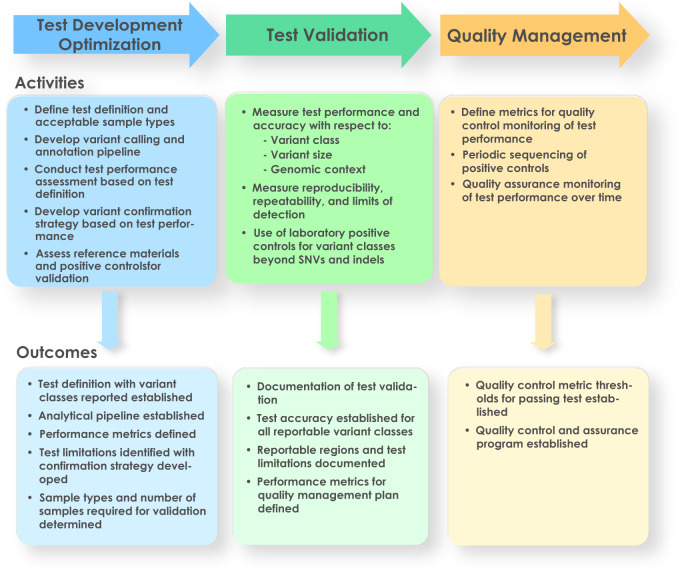
Whole-genome sequencing (WGS) has shown promise in becoming a first-tier diagnostic test for patients with rare genetic disorders; however, standards addressing the definition and deployment practice of a best-in-class test are lacking. To address these gaps, the Medical Genome Initiative, a consortium of leading healthcare and research organizations in the US and Canada, was formed to expand access to high-quality clinical WGS by publishing best practices. Here, we present consensus recommendations on clinical WGS analytical validation for the diagnosis of individuals with suspected germline disease with a focus on test development, upfront considerations for test design, test validation practices, and metrics to monitor test performance. This work also provides insight into the current state of WGS testing at each member institution, including the utilization of reference and other standards across sites. Importantly, members of this initiative strongly believe that clinical WGS is an appropriate first-tier test for patients with rare genetic disorders, and at minimum is ready to replace chromosomal microarray analysis and whole-exome sequencing. The recommendations presented here should reduce the burden on laboratories introducing WGS into clinical practice, and support safe and effective WGS testing for diagnosis of germline disease.
Keywords: Genetic testing; Laboratory techniques and procedures; Next-generation sequencing.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsS.L.T., R.J.T., and J.W.B. are current employees and shareholders of Illumina Inc.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
