

Acute zonal occult outer retinopathy presenting as optic neuritis
- PMID: 33110756
- PMCID: PMC7585482
- DOI: 10.4103/tjo.tjo_11_20
Acute zonal occult outer retinopathy presenting as optic neuritis
Abstract
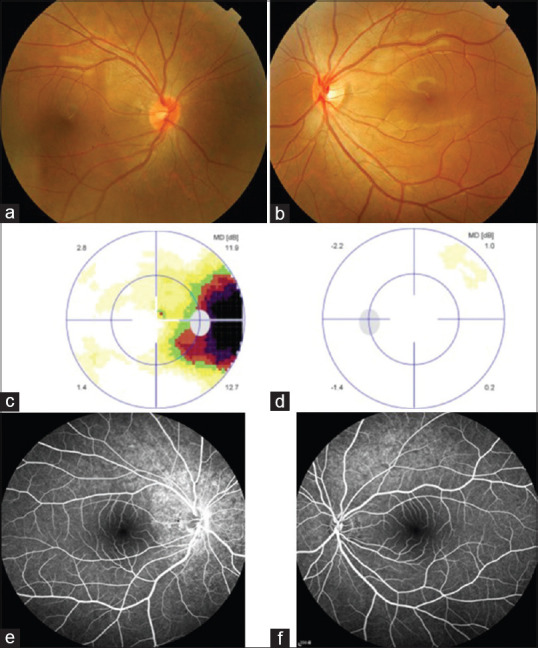
Acute zonal occult outer retinopathy (AZOOR) is an outer retinal disorder characterized by the acute loss of visual functions. Herein, we report a case of AZOOR presenting features mimicking optic neuritis. A 17-year-old healthy male reported fogginess in the right eye for 2 weeks. His best-corrected visual acuity was 20/20 in both eyes. Results of a color vision test and pupillary reaction were unremarkable. Funduscopic examination revealed a subtle hyperemic disc surrounded by hyperpigmentation in the right eye. Visual field examination confirmed an enlarged blind spot in the affected eye. Fundus autofluorescence imaging revealed zonal hyperautofluorescence around the optic disc. Fluorescein angiography showed optic disc staining and a window defect in the retinal pigment epithelium. Optical coherence tomography demonstrated loss of the ellipsoid line at the corresponding hyperautofluorescent region. All these characteristics indicated a diagnosis of AZOOR. However, the prolonged P100 wave observed through visual-evoked potential examination, hyperintensity T2 signal at the retrobulbar optic nerve through magnetic resonance imaging, and mild hyperemic optic disc along with optic disc staining through fluorescein angiography resemble the characteristics of optic neuritis. Because the clinical features of AZOOR are similar to those of optic neuritis, ophthalmologists should be able to differentiate between these two diseases to achieve a timely and correct diagnosis.
Keywords: Autofluorescence; acute zonal occult outer retinopathy; optic neuritis; optical coherence tomography.
Copyright: © 2020 Taiwan J Ophthalmol.
Conflict of interest statement
The authors declare that there are no conflicts of interests of this article.
Figures




References
-
- Gass JD. Acute zonal occult outer retinopathy.Donders lecture: The Netherlands ophthalmological society, Maastricht, Holland, June 19, 1992. J Clin Neuroophthalmol. 1993;13:79–97. - PubMed
-
- Gass JD, Agarwal A, Scott IU. Acute zonal occult outer retinopathy: A long-term follow-up study. Am J Ophthalmol. 2002;134:329–39. - PubMed
-
- Jacobson DM. Acute zonal occult outer retinopathy and central nervous system inflammation. J Neuroophthalmol. 1996;16:172–7. - PubMed
-
- Khaleeli Z, Tucker WR, Del Porto L, Virgo JD, Plant GT. Remember the retina: Retinal disorders presenting to neurologists. Pract Neurol. 2018;18:84–96. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases