

Comparison of Structural Subscapularis Integrity After Latarjet Procedure Versus Iliac Crest Bone Graft Transfer
- PMID: 33110928
- PMCID: PMC7564622
- DOI: 10.1177/2325967120958007
Comparison of Structural Subscapularis Integrity After Latarjet Procedure Versus Iliac Crest Bone Graft Transfer
Abstract
Background: Although clinical outcome scores are comparable after coracoid transfer procedure (Latarjet) and iliac crest bone graft transfer (ICBGT) for anterior shoulder instability with glenoid bone loss, a significant decrease in internal rotation capacity has been reported for the Latarjet procedure.
Hypothesis: The subscapularis (SSC) musculotendinous integrity will be less compromised by ICBGT than by the Latarjet procedure.
Study design: Cohort study; Level of evidence, 3.
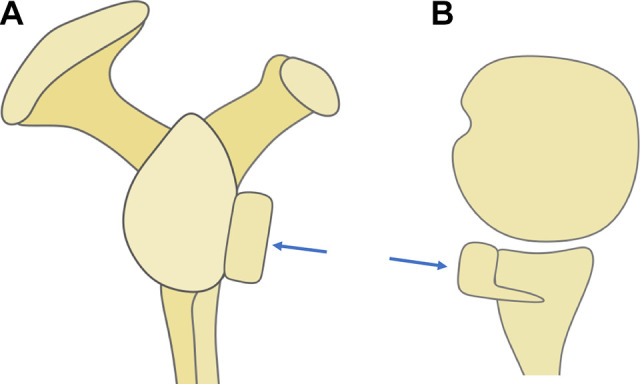
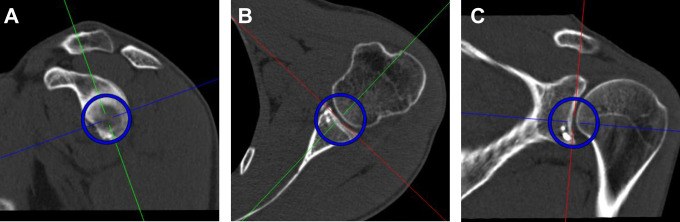
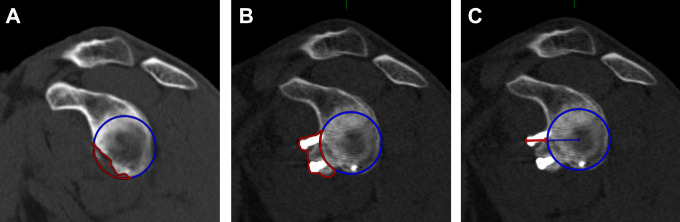
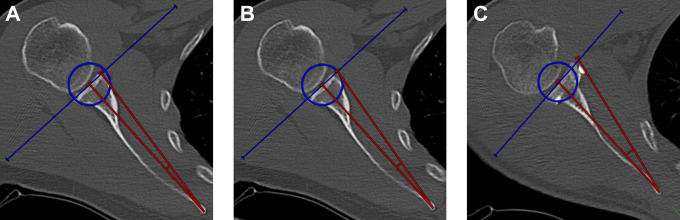
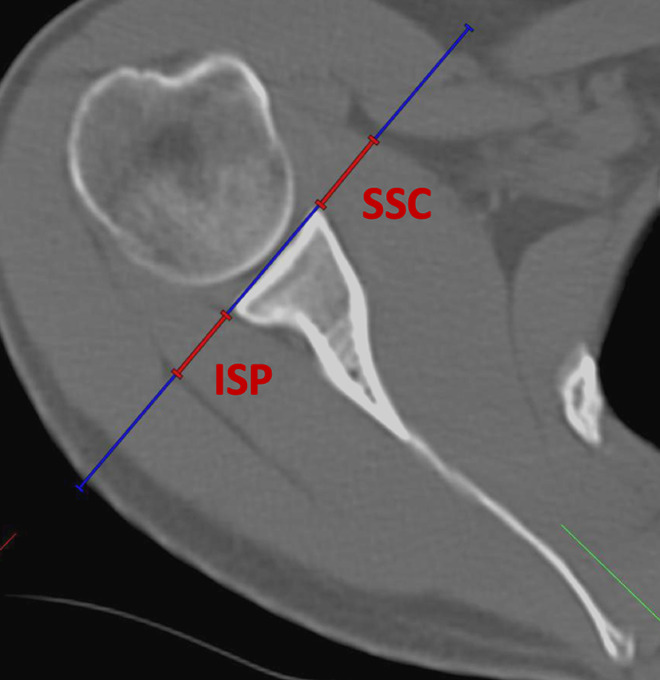
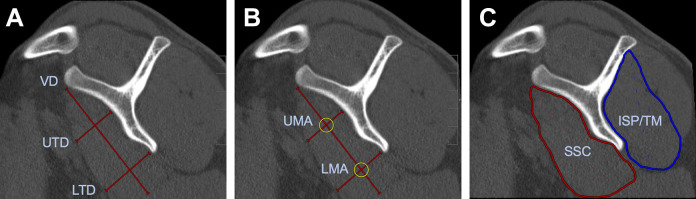
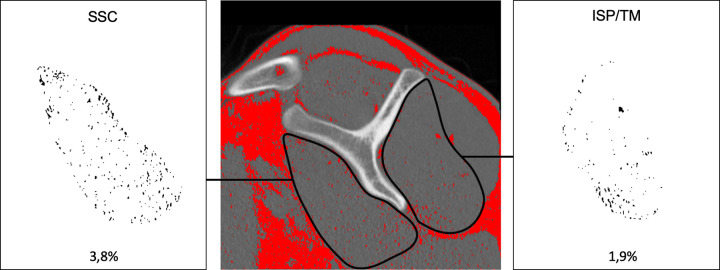
Methods: We retrospectively analyzed pre- and postoperative computed tomography (CT) scans at short-term follow-up of 52 patients (26 Latarjet, 26 ICBGT) previously assessed in a prospective randomized controlled trial. Measurements included the preoperative glenoid defect area and graft area protruding the glenoid rim at follow-up and tendon thickness assessed through SSC and infraspinatus (ISP) ratios. Fatty muscle infiltration was graded according to Goutallier, quantified with muscle attenuation in Hounsfield units, and additionally calculated as percentages. We measured 3 angles to describe rerouting of the SSC musculotendinous unit around the bone grafts.
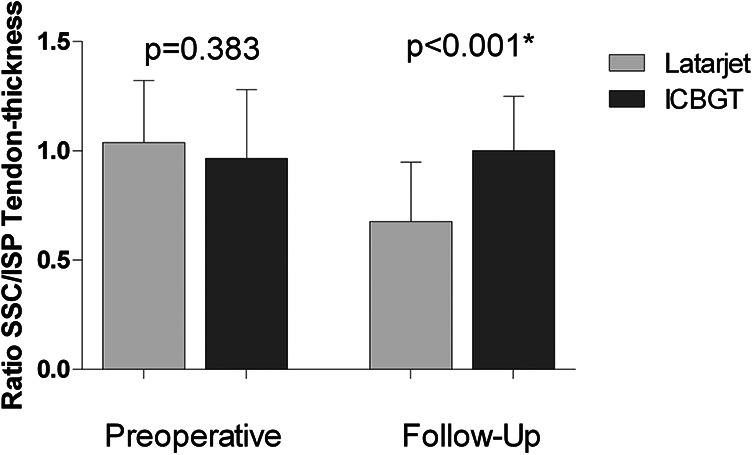
Results: SSC fatty muscle infiltration was 2.0% ± 2.2% in the Latarjet group versus 2.4% ± 2.2% in ICBGT (P = .546) preoperatively and showed significantly higher values in the Latarjet group at follow-up (5.3% ± 4.5% vs 2.3% ± 1.7%; P = .001). In total, 4 patients (15.4%) in the Latarjet group showed a progression from grade 0 to grade 1 at follow-up, whereas no changes in the ICBGT group were noted. The measured rerouting angle of the SSC muscle was significantly increased in the Latarjet group (11.8° ± 2.1°) compared with ICBGT (7.5° ± 1.3°; P < .001) at follow-up, with a significant positive correlation between this angle and fatty muscle infiltration (R = 0.447; P = .008). Ratios of SSC/ISP tendon thickness were 1.03 ± 0.3 in the Latarjet group versus 0.97 ± 0.3 (P = .383) in ICBGT preoperatively and showed significantly lower ratios in the Latarjet group (0.7 ± 0.3 vs 1.0 ± 0.2; P < .001) at follow-up.
Conclusion: Although clinical outcome scores after anterior shoulder stabilization with a Latarjet procedure and ICBGT are comparable, this study shows that the described decline in internal rotation capacity after Latarjet procedure has a radiographic structural correlate in terms of marked thinning and rerouting of the SSC tendon as well as slight fatty degeneration of the muscle.
Keywords: Latarjet; iliac crest bone graft transfer; shoulder instability; subscapularis.
© The Author(s) 2020.
Conflict of interest statement
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Anderl W, Pauzenberger L, Laky B, Kriegleder B, Heuberer PR. Arthroscopic implant-free bone grafting for shoulder instability with glenoid bone loss: clinical and radiological outcome at a minimum 2-year follow-up. Am J Sports Med. 2016;44(5):1137–1145. - PubMed
-
- Auffarth A, Schauer J, Matis N, et al. The J-bone graft for anatomical glenoid reconstruction in recurrent posttraumatic anterior shoulder dislocation. Am J Sports Med. 2008;36(4):638–647. - PubMed
-
- Baudi P, Righi P, Bolognesi D, et al. How to identify and calculate glenoid bone deficit. Chir Organi Mov. 2005;90(2):145–152. - PubMed
-
- Burkhart SS, De Beer JF. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16(7):677–694. - PubMed
LinkOut - more resources
Full Text Sources
