

24-Month Outcomes of Primary Care Web-Based Depression Prevention Intervention in Adolescents: Randomized Clinical Trial
- PMID: 33112254
- PMCID: PMC7657722
- DOI: 10.2196/16802
24-Month Outcomes of Primary Care Web-Based Depression Prevention Intervention in Adolescents: Randomized Clinical Trial
Abstract
Background: Adolescent depression carries a high burden of disease worldwide, but access to care for this population is limited. Prevention is one solution to curtail the negative consequences of adolescent depression. Internet interventions to prevent adolescent depression can overcome barriers to access, but few studies examine long-term outcomes.
Objective: This study compares CATCH-IT (Competent Adulthood Transition with Cognitive Behavioral Humanistic and Interpersonal Training), an internet-based intervention, to a general health education active control for depression onset at 12 and 24 months in adolescents presenting to primary care settings.
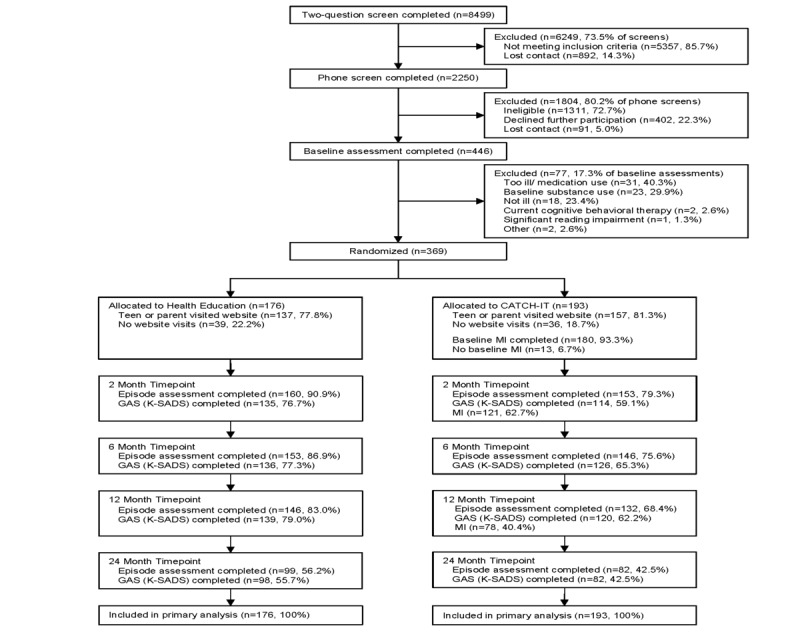
Methods: A 2-site randomized trial, blinded to the principal investigators and assessors, was conducted comparing Competent Adulthood Transition with Cognitive Behavioral Humanistic and Interpersonal Training to health education to prevent depressive episodes in 369 adolescents (193 youths were randomly assigned to Competent Adulthood Transition with Cognitive Behavioral Humanistic and Interpersonal Training and 176 to health education) with subthreshold depressive symptoms or prior depressive episodes. Participants were recruited from primary care settings in the United States. The primary outcome was the occurrence of a depressive episode, determined by the Depression Symptom Rating. The secondary outcome was functioning, measured by the Global Assessment Scale.
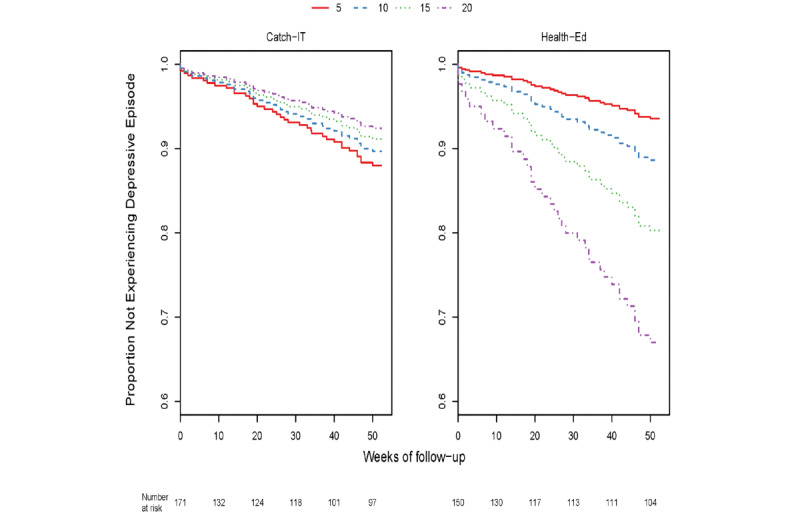
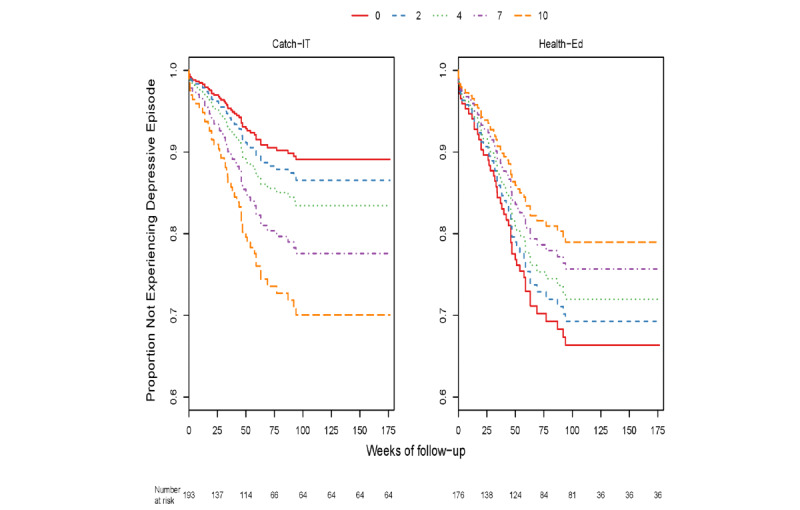
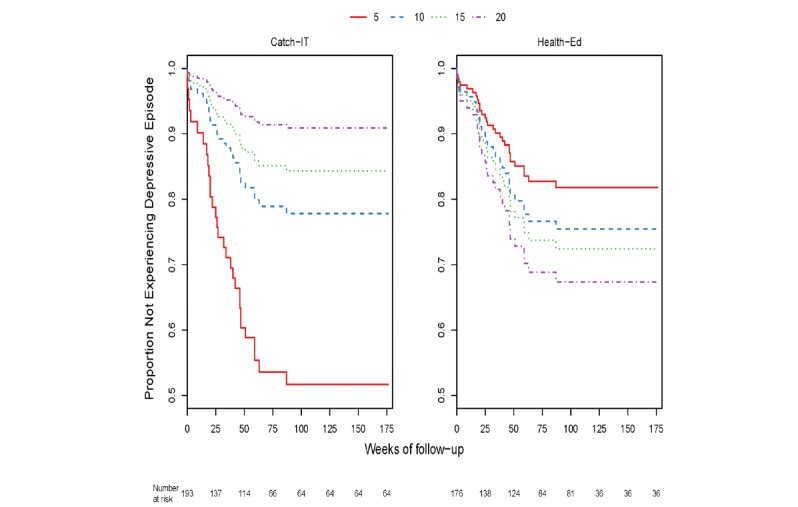
Results: In intention-to-treat analyses, the adjusted hazard ratio favoring Competent Adulthood Transition with Cognitive Behavioral Humanistic and Interpersonal Training for first depressive episode was not statistically significant at 12 months (hazard ratio 0.77, 95% CI 0.42-1.40, P=.39) and 24 months (hazard ratio 0.87, 95% CI 0.52-1.47, P=.61). Competent Adulthood Transition with Cognitive Behavioral Humanistic and Interpersonal Training provided preventive benefit for first depressive episode for those with mild hopelessness or at least moderate paternal monitoring at baseline. Global Assessment Scale scores improved comparably in both groups (intention-to-treat).
Conclusions: A technology-based intervention for adolescent depression prevention implemented in primary care did not have additional benefit at 12 or 24 months. Further research is necessary to determine whether internet interventions have long-term benefit.
Trial registration: ClinicalTrials.gov NCT01893749; http://clinicaltrials.gov/ct2/show/NCT01893749.
Keywords: adolescent; depression; eHealth; prevention; scalable.
©Benjamin Van Voorhees, Tracy R G Gladstone, Kunmi Sobowale, C Hendricks Brown, David A Aaby, Daniela A Terrizzi, Jason Canel, Eumene Ching, Anita D Berry, James Cantorna, Milton Eder, William Beardslee, Marian Fitzgibbon, Monika Marko-Holguin, Linda Schiffer, Miae Lee, Sarah A de Forest, Emily E Sykes, Jennifer H Suor, Theodore J Crawford, Katie L Burkhouse, Brady C Goodwin, Carl Bell. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 28.10.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Randomized Clinical Trial of an Internet-Based Adolescent Depression Prevention Intervention in Primary Care: Internalizing Symptom Outcomes.Int J Environ Res Public Health. 2020 Oct 22;17(21):7736. doi: 10.3390/ijerph17217736. Int J Environ Res Public Health. 2020. PMID: 33105889 Free PMC article. Clinical Trial.
-
An internet-based adolescent depression preventive intervention: study protocol for a randomized control trial.Trials. 2015 May 1;16:203. doi: 10.1186/s13063-015-0705-2. Trials. 2015. PMID: 25927539 Free PMC article. Clinical Trial.
-
Effect of Internet-based Cognitive Behavioral Humanistic and Interpersonal Training vs. Internet-based General Health Education on Adolescent Depression in Primary Care: A Randomized Clinical Trial.JAMA Netw Open. 2018 Nov;1(7):e184278. doi: 10.1001/jamanetworkopen.2018.4278. JAMA Netw Open. 2018. PMID: 30533601 Free PMC article.
-
Nonsomatic treatment of depression.Child Adolesc Psychiatr Clin N Am. 2002 Jul;11(3):579-93. doi: 10.1016/s1056-4993(02)00009-3. Child Adolesc Psychiatr Clin N Am. 2002. PMID: 12222084 Review.
-
How do eHealth Programs for Adolescents With Depression Work? A Realist Review of Persuasive System Design Components in Internet-Based Psychological Therapies.J Med Internet Res. 2017 Aug 9;19(8):e266. doi: 10.2196/jmir.7573. J Med Internet Res. 2017. PMID: 28793983 Free PMC article. Review.
Cited by
-
Understanding Mobile Health and Youth Mental Health: Scoping Review.JMIR Mhealth Uhealth. 2023 Jun 16;11:e44951. doi: 10.2196/44951. JMIR Mhealth Uhealth. 2023. PMID: 37220197 Free PMC article.
-
Randomized Clinical Trial of an Internet-Based Adolescent Depression Prevention Intervention in Primary Care: Internalizing Symptom Outcomes.Int J Environ Res Public Health. 2020 Oct 22;17(21):7736. doi: 10.3390/ijerph17217736. Int J Environ Res Public Health. 2020. PMID: 33105889 Free PMC article. Clinical Trial.
-
Short Video-Based Mental Health Intervention for Depressive Symptoms in Junior High School Students: A Cluster Randomized Controlled Trial.Psychol Res Behav Manag. 2023 Oct 16;16:4169-4181. doi: 10.2147/PRBM.S433467. eCollection 2023. Psychol Res Behav Manag. 2023. PMID: 37868654 Free PMC article.
-
Evaluating the necessity of booster sessions in relapse prevention for depression: a longitudinal study.Front Psychol. 2025 Jun 24;16:1568141. doi: 10.3389/fpsyg.2025.1568141. eCollection 2025. Front Psychol. 2025. PMID: 40631058 Free PMC article.
-
Role of social innovations in health in the prevention and control of infectious diseases: a scoping review.Infect Dis Poverty. 2024 Nov 20;13(1):87. doi: 10.1186/s40249-024-01253-w. Infect Dis Poverty. 2024. PMID: 39563417 Free PMC article.
References
-
- Bromet E, Andrade LH, Hwang I, Sampson NA, Alonso J, de Girolamo Giovanni, de Graaf Ron, Demyttenaere K, Hu C, Iwata N, Karam AN, Kaur J, Kostyuchenko S, Lépine Jean-Pierre, Levinson D, Matschinger H, Mora MEM, Browne MO, Posada-Villa J, Viana MC, Williams DR, Kessler RC. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011 Jul 26;9:90. doi: 10.1186/1741-7015-9-90. https://bmcmedicine.biomedcentral.com/articles/10.1186/1741-7015-9-90 - DOI - DOI - PMC - PubMed
-
- Janssens KAM, Rosmalen JGM, Ormel J, van Oort FVA, Oldehinkel AJ. Anxiety and depression are risk factors rather than consequences of functional somatic symptoms in a general population of adolescents: the TRAILS study. J Child Psychol Psychiatry. 2010 Mar;51(3):304–12. doi: 10.1111/j.1469-7610.2009.02174.x. - DOI - PubMed
-
- Pettit J W, Lewinsohn P M, Roberts R E, Seeley J R, Monteith L. The long-term course of depression: development of an empirical index and identification of early adult outcomes. Psychol Med. 2009 Mar;39(3):403–12. doi: 10.1017/S0033291708003851. http://europepmc.org/abstract/MED/18606049 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
