

Value of Coronary Artery Calcium Scanning in Association With the Net Benefit of Aspirin in Primary Prevention of Atherosclerotic Cardiovascular Disease
- PMID: 33112372
- PMCID: PMC7593878
- DOI: 10.1001/jamacardio.2020.4939
Value of Coronary Artery Calcium Scanning in Association With the Net Benefit of Aspirin in Primary Prevention of Atherosclerotic Cardiovascular Disease
Erratum in
-
Error in Author Degree.JAMA Cardiol. 2021 Feb 1;6(2):246. doi: 10.1001/jamacardio.2020.6736. JAMA Cardiol. 2021. PMID: 33325997 Free PMC article. No abstract available.
Abstract
Importance: Higher coronary artery calcium (CAC) identifies individuals at increased atherosclerotic cardiovascular disease (ASCVD) risk. Whether it can also identify individuals likely to derive net benefit from aspirin therapy is unclear.
Objective: To examine the association between CAC, bleeding, and ASCVD and explore the net estimated effect of aspirin at different CAC thresholds.
Design, setting, and participants: Prospective population-based cohort study of Dallas Heart Study participants, free from ASCVD and not taking aspirin at baseline. Data were analyzed between February 1, 2020, and July 15, 2020.
Exposures: Coronary artery calcium score in the following categories: 0, 1-99, and 100 or higher.
Main outcomes and measures: Major bleeding and ASCVD events were identified from International Statistical Classification of Diseases and Related Health Problems, Ninth Revision codes. Meta-analysis-derived aspirin effect estimates were applied to observed ASCVD and bleeding rates to model the net effect of aspirin at different CAC thresholds.
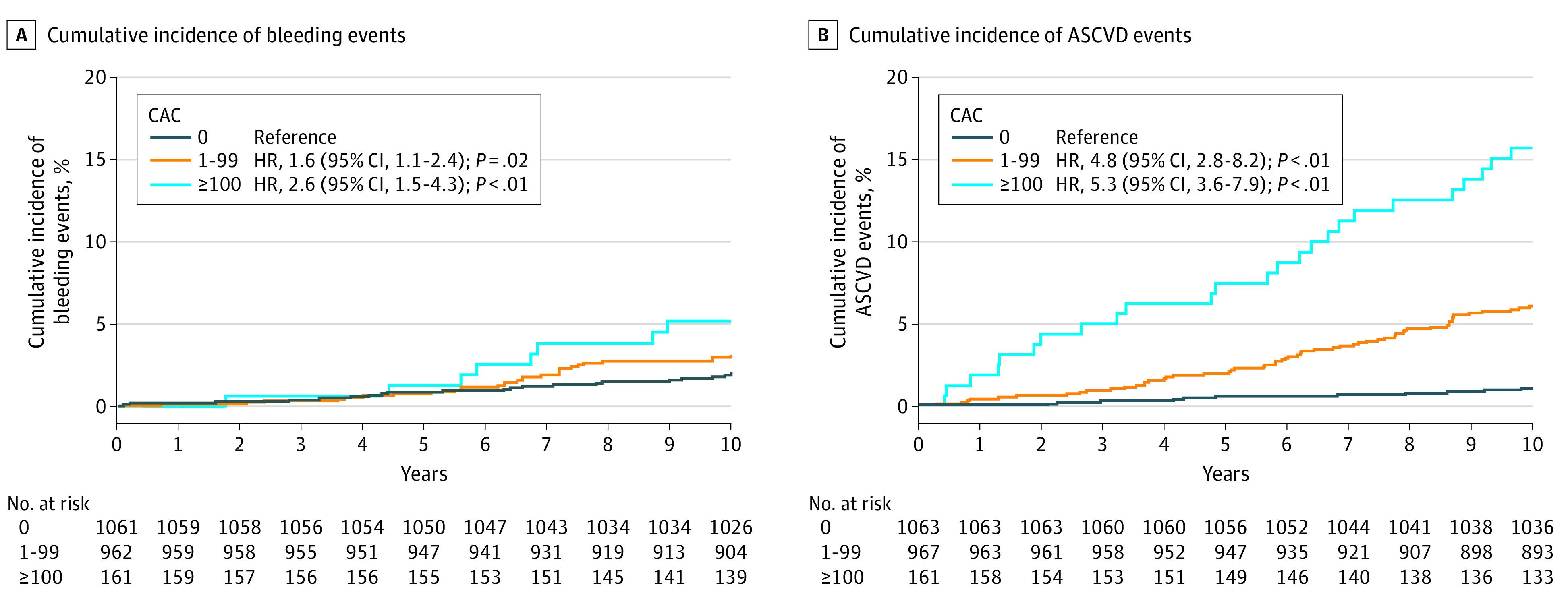
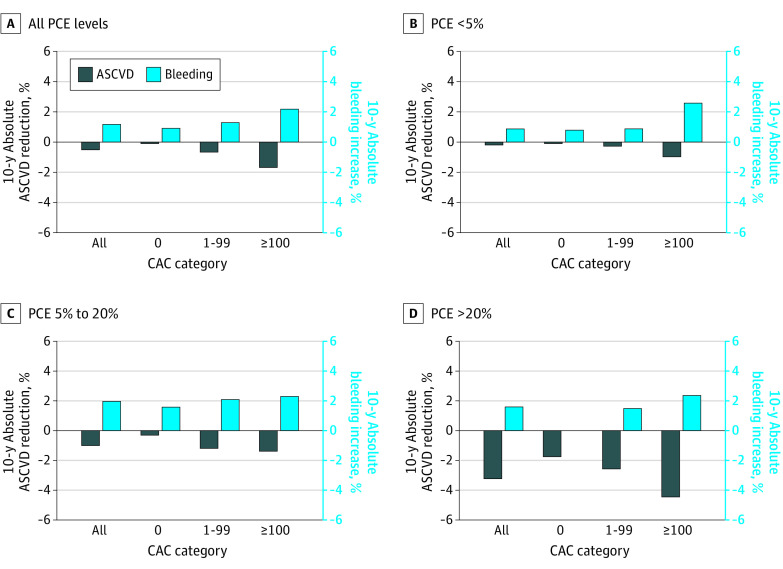
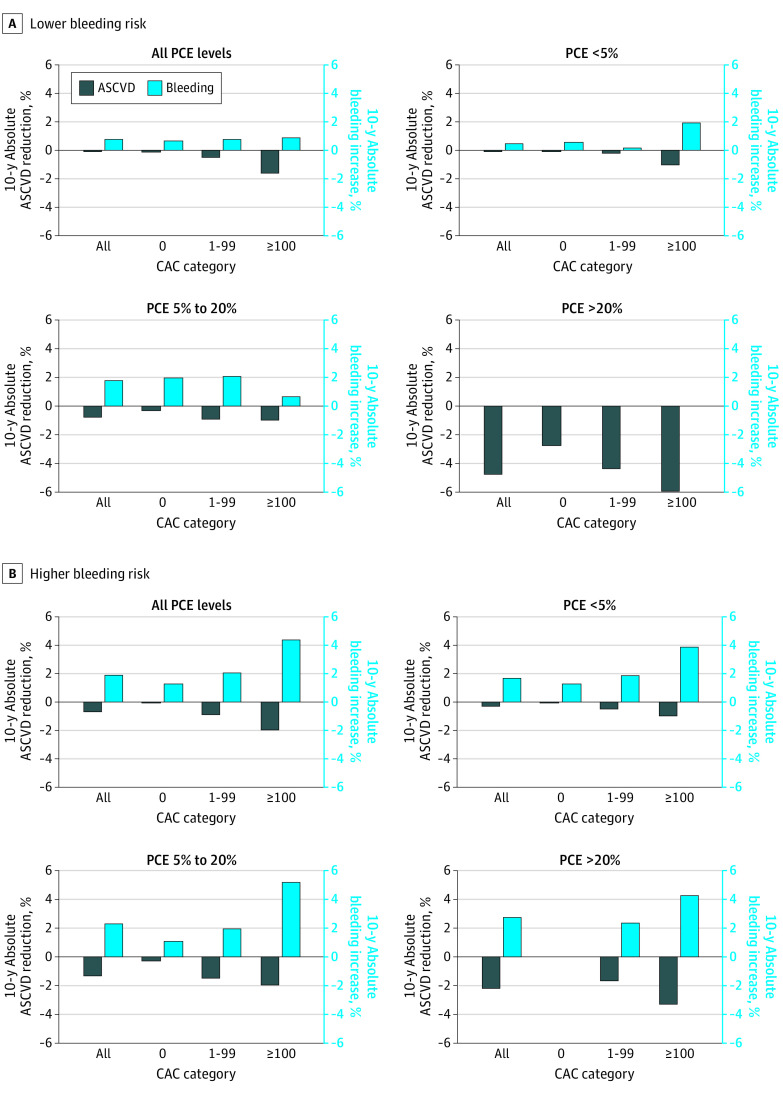
Results: A total of 2191 participants (mean [SD], age 44 [9.1] years, 1247 women [57%], and 1039 black individuals [47%]) had 116 major bleeding and 123 ASCVD events over a median follow-up of 12.2 years. Higher CAC categories (CAC 1-99 and ≥100 vs CAC 0) were associated with both ASCVD and bleeding events (hazard ratio [HR], 1.6; 95% CI, 1.1-2.4; HR, 2.6; 95% CI, 1.5-4.3; HR, 4.8; 95% CI, 2.8-8.2; P < .001; HR, 5.3; 95% CI, 3.6-7.9; P < .001), but the association between CAC and bleeding was attenuated after multivariable adjustment. Applying meta-analysis estimates, irrespective of CAC, aspirin use was estimated to result in net harm in individuals at low (<5%) and intermediate (5%-20%) 10-year ASCVD risk and net benefit in those at high (≥20%) ASCVD risk. Among individuals at lower bleeding risk, a CAC score of at least 100 identified individuals who would experience net benefit, but only in those at borderline or higher (≥5%) 10-year ASCVD risk. In individuals at higher bleeding risk, there would be net harm from aspirin irrespective of CAC and ASCVD risk.
Conclusions and relevance: Higher CAC is associated with both ASCVD and bleeding events, with a stronger association with ASCVD. A high CAC score identifies individuals estimated to derive net benefit from primary prevention aspirin therapy from those who would not, but only in the setting of lower bleeding risk and estimated ASCVD risk that is not low.
Conflict of interest statement
Figures
Comment in
-
Coronary Artery Calcium for Personalized Risk Management-A Second Chance for Aspirin in Primary Prevention?JAMA Cardiol. 2021 Feb 1;6(2):187-188. doi: 10.1001/jamacardio.2020.4961. JAMA Cardiol. 2021. PMID: 33112364 No abstract available.
References
-
- Baigent C, Blackwell L, Collins R, et al. ; Antithrombotic Trialists’ (ATT) Collaboration . Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373(9678):1849-1860. doi: 10.1016/S0140-6736(09)60503-1 - DOI - PMC - PubMed
-
- Gaziano JM, Brotons C, Coppolecchia R, et al. ; ARRIVE Executive Committee . Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet. 2018;392(10152):1036-1046. doi: 10.1016/S0140-6736(18)31924-X - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
