

Evolving Trends in Adult Heart Transplant With the 2018 Heart Allocation Policy Change
- PMID: 33112391
- PMCID: PMC7593876
- DOI: 10.1001/jamacardio.2020.4909
Evolving Trends in Adult Heart Transplant With the 2018 Heart Allocation Policy Change
Abstract
Importance: The US heart allocation policy was changed on October 18, 2018. The association of this change with recipient and donor selection and outcomes remains to be elucidated.
Objective: To evaluate changes in patient characteristics, wait list outcomes, and posttransplant outcomes after the recent allocation policy change in heart transplant.
Design, setting, and participants: In this cohort study, all 15 631 adults undergoing heart transplants, excluding multiorgan transplants, in the US as identified by the United Network for Organ Sharing multicenter, national registry were reviewed. Patients were stratified according to prepolicy change (October 1, 2015, to October 1, 2018) and postpolicy change (October 18, 2018 or after). Follow-up data were available through March 31, 2020.
Exposures: Heart transplants after the policy change.
Main outcomes and measures: Competing risk regression for wait list outcomes was performed. Posttransplant survival was compared using the Kaplan-Meier method, and risk adjustment was performed using multivariable Cox proportional hazards regression analysis.
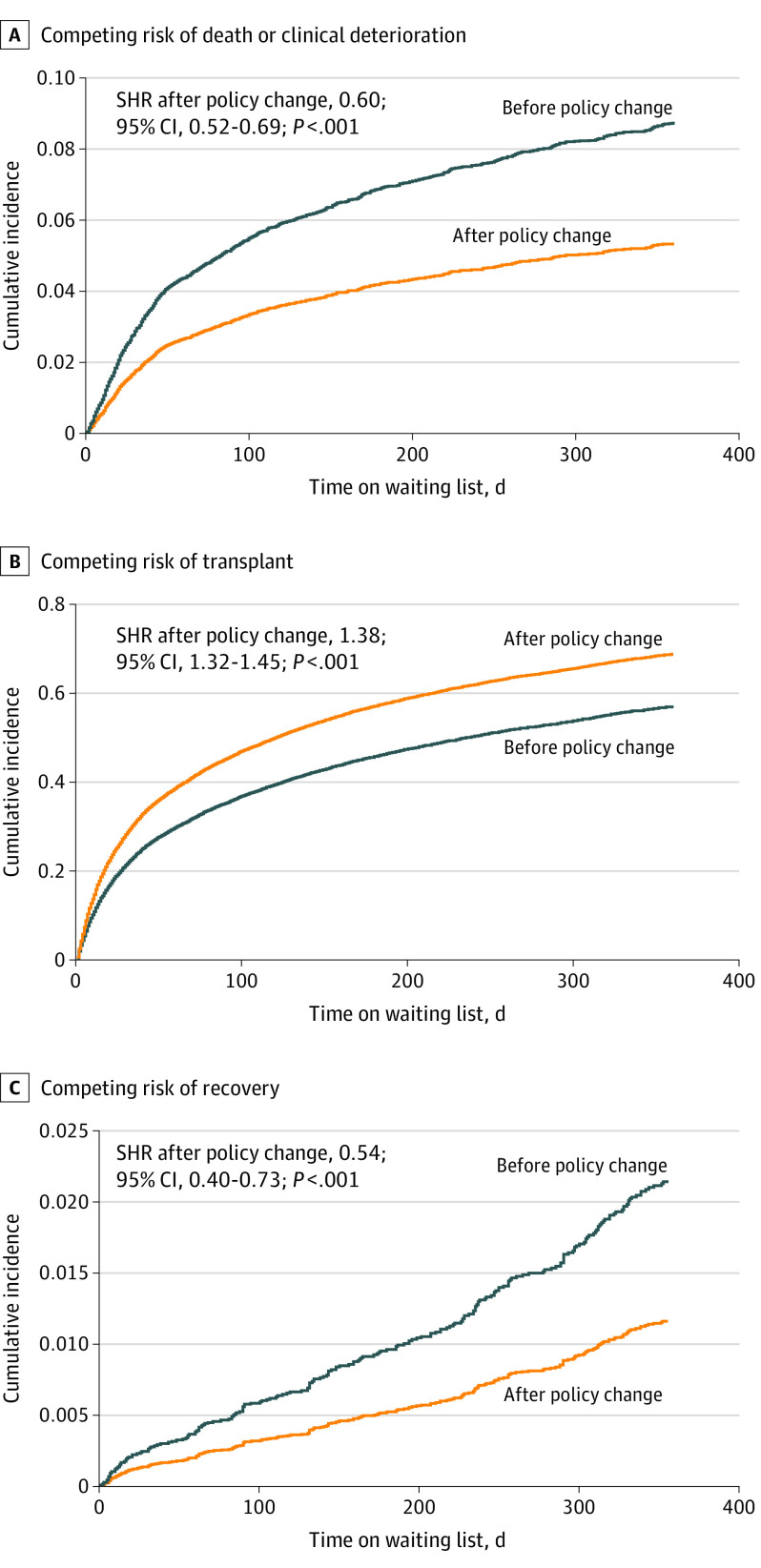
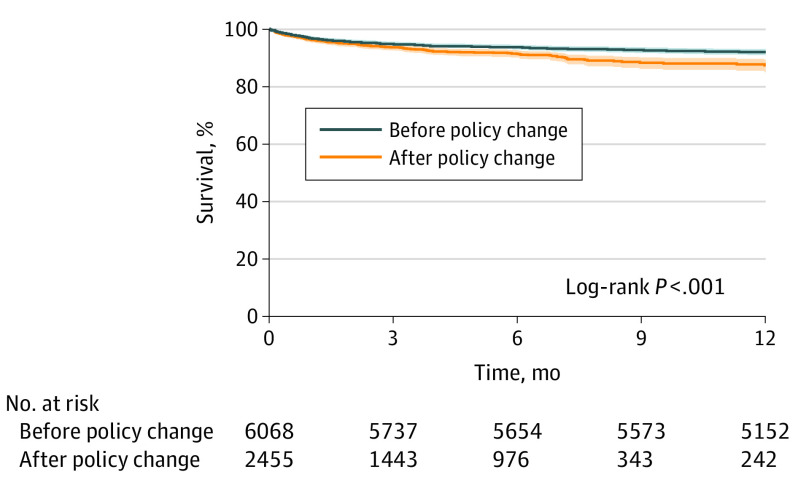
Results: In this cohort study, of the 15 631 patients undergoing transplant, 10 671 (mean [SD] age, 53.1 [12.7] years; 7823 [73.3%] male) were wait listed before and 4960 (mean [SD] age, 52.7 [13.0] years; 3610 [72.8%] male) were wait listed after the policy change. Competing risk regression demonstrated reduced likelihood of mortality or deterioration (subhazard ratio [SHR], 0.60; 95% CI, 0.52-0.69; P < .001), increased likelihood of transplant (SHR, 1.38; 95% CI, 1.32-1.45; P < .001), and reduced likelihood of recovery (SHR, 0.54; 95% CI, 0.40-0.73; P < .001) for wait listed patients after the policy change. A total of 6078 patients underwent transplant before and 2801 after the policy change. Notable changes after the policy change included higher frequency of bridging with temporary mechanical circulatory support and lower frequency of bridging with durable left ventricular assist devices. Posttransplant survival was reduced after the policy change (1-year: 92.1% vs 87.5%; log-rank P < .001), a finding that persisted after risk adjustment (HR, 1.29; 95% CI, 1.07-1.55; P = .008).
Conclusions and relevance: Substantial changes have occurred in adult heart transplant in the US after the policy change in October 2018. Wait list outcomes have improved, although posttransplant survival has decreased. These data confirm findings from earlier preliminary analyses and demonstrate that these trends have persisted to 1-year follow-up, underscoring the importance of continued reevaluation of the new heart allocation policy.
Conflict of interest statement
Figures
Comment in
-
United Network for Organ Sharing 2018 Heart Transplant Reallocation Policy: Aiming for Evidence-Based Policy.JAMA Cardiol. 2021 Feb 1;6(2):168. doi: 10.1001/jamacardio.2020.5232. JAMA Cardiol. 2021. PMID: 33112392 No abstract available.
References
-
- Organ Procurement and Transplantation Network Adult Heart Allocation. Accessed March 22, 2020. https://optn.transplant.hrsa.gov/learn/professional-education/adult-hear...
-
- Fine JP, Gray RJ. A proportional hazards model for the subdistribution of competing risks in survival analysis. J Am Stat Assoc. 1999;94:496-509. doi: 10.1080/01621459.1999.10474144 - DOI
-
- Schulze PC, Kitada S, Clerkin K, Jin Z, Mancini DM. Regional differences in recipient waitlist time and pre- and post-transplant mortality after the 2006 United Network for Organ Sharing policy changes in the donor heart allocation algorithm. JACC Heart Fail. 2014;2(2):166-177. doi: 10.1016/j.jchf.2013.11.005 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
