

IGF1 for the diagnosis of growth hormone deficiency in children and adolescents: a reappraisal
- PMID: 33112822
- PMCID: PMC7774770
- DOI: 10.1530/EC-20-0347
IGF1 for the diagnosis of growth hormone deficiency in children and adolescents: a reappraisal
Abstract
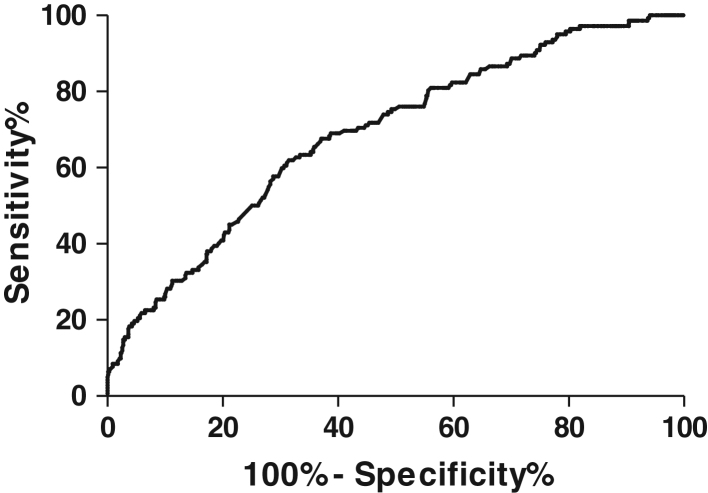
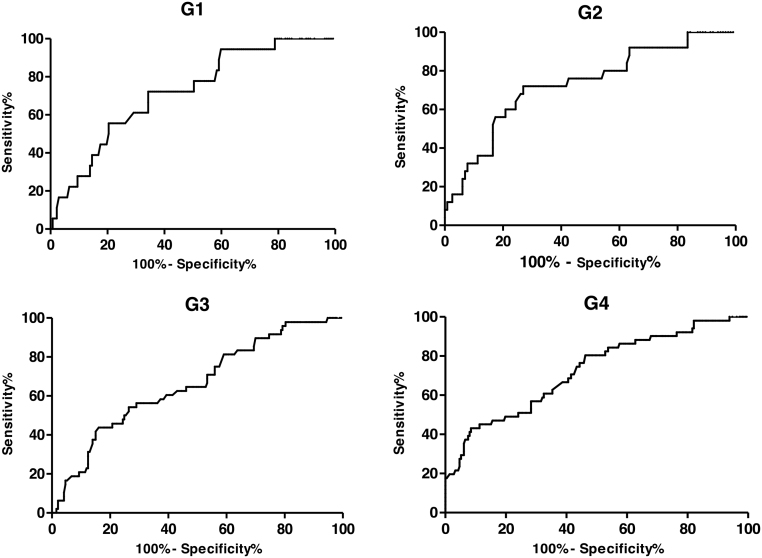
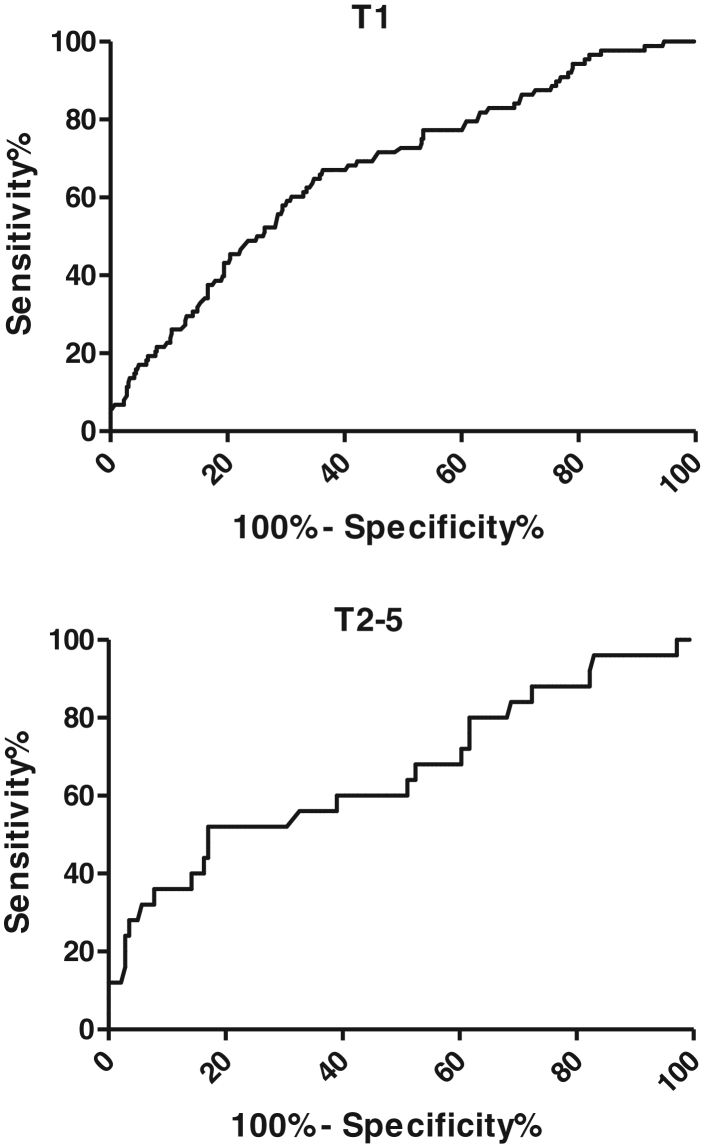
A number of studies have evaluated the role of IGF1 measurement in the diagnosis of growth hormone deficiency (GHD). This study aimed to evaluate the accuracy and the best cut-off of IGF1 SDS in the diagnosis of GHD in a large cohort of short children and adolescents. One-hundred and forty-two children and adolescents with GHD ((63 organic/genetic (OGHD), 79 idiopathic (IGHD)) and 658 short non-GHD children (median age 10.4 years) were included in the analysis. The two groups were subdivided according to age (G1 <6, G2 6 <9, G3 9 <12, G4 ≥12) and to pubertal status. Serum IGFI was measured by the same chemiluminescence assay in all samples and expressed as age- and sex-based SDS. Receiver operating characteristic (ROC) analysis was used to evaluate the optimal IGF1 SDS cut-off and the diagnostic accuracy. Median IGF1 SDS was significantly lower in the GHD than in non-GHD patients. The area under the curve (AUC) was 0.69, with the best IGF1 cut-off of -1.5 SDS (sensitivity 67.61%, specificity 62.62%). The AUC was 0.75 for OGHD and 0.63 for IGHD. The accuracy was better in the pubertal (AUC = 0.81) than the prepubertal group (AUC = 0.64). In our cohort, IGF1 measurement has poor accuracy in discriminating GHD from non-GHD. Our findings confirm and reinforce the belief that IGF1 values should not be used alone in the diagnosis of GHD but should be interpreted in combination with other clinical and biochemical parameters.
Keywords: adolescents; children; growth hormone deficiency; insulin-like growth factor 1; short stature.
Figures
References
-
- Collett-Solberg PF, Ambler G, Backeljauw PF, Bidlingmaier M, Biller BMK, Boguszewski MCS, Cheung PT, Choong CSY, Cohen LE, Cohen P.et al Diagnosis, genetics, and therapy of short stature in children: a Growth Hormone Research Society International Perspective. Hormone Research in Paediatrics 2019. 92 1–14. (10.1159/000502231) - DOI - PMC - PubMed
-
- Cohen P, Rogol AD, Deal CL, Saenger P, Reiter EO, Ross JL, Chernausek SD, Savage MO, Wit JM.2007 ISS Consensus Workshop participants. Consensus statement on the diagnosis and treatment of children with idiopathic short stature: a summary of the Growth Hormone Research Society, the Lawson Wilkins Pediatric Endocrine Society, and the European Society for Paediatric Endocrinology Workshop. Journal of Clinical Endocrinology and Metabolism 2008. 93 4210–4217. (10.1210/jc.2008-0509) - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
