

Impact of serum and follicular fluid kisspeptin and estradiol on oocyte maturity and endometrial thickness among unexplained infertile females during ICSI
- PMID: 33112855
- PMCID: PMC7593084
- DOI: 10.1371/journal.pone.0239142
Impact of serum and follicular fluid kisspeptin and estradiol on oocyte maturity and endometrial thickness among unexplained infertile females during ICSI
Abstract
Objective: To relate serum and follicular fluid (FF) kisspeptin and estradiol levels in different stages of stimulation during Intracytoplasmic Sperm Injection (ICSI) with oocyte maturity and endometrial thickness among unexplained infertile females.
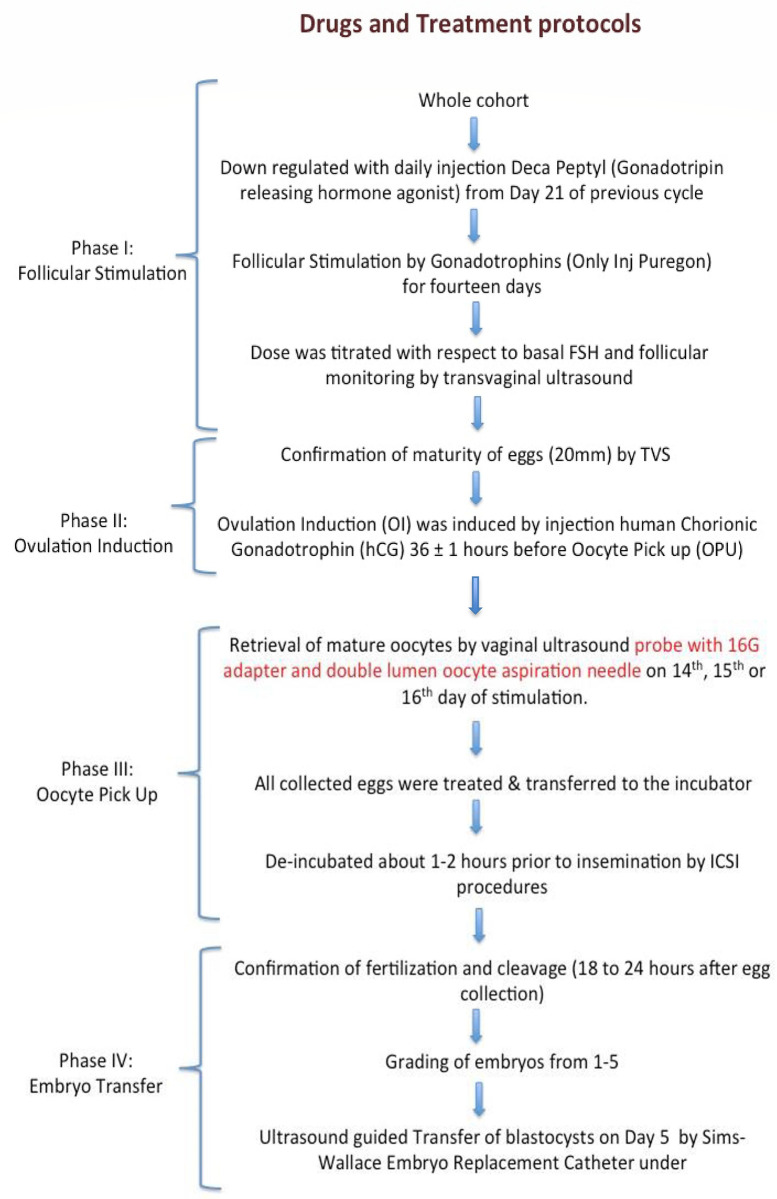
Methods: This cross-sectional study was carried out at the Australian Concept Infertility Medical Centre from March 2017 till March 2018. Fifty unexplained infertile females, booked for ICSI, were included in the study. Serum kisspeptin and estradiol were estimated by Enzyme-Linked Immunosorbent Assay in all four stages; 1: follicular stimulation, 2: ovulation induction, 3: oocyte pickup, and 4: embryo transfer. FF was aspirated during oocyte retrieval (stage 3) for the analysis of KP and estradiol. Pregnancy outcomes were categorized as non-pregnant, preclinical abortion, and clinical pregnancy.
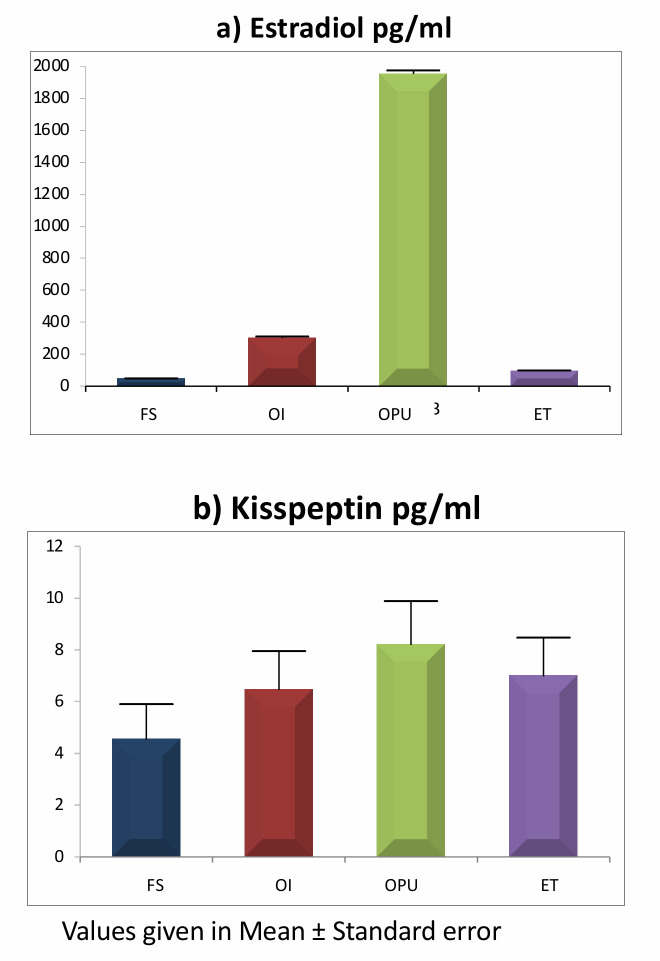
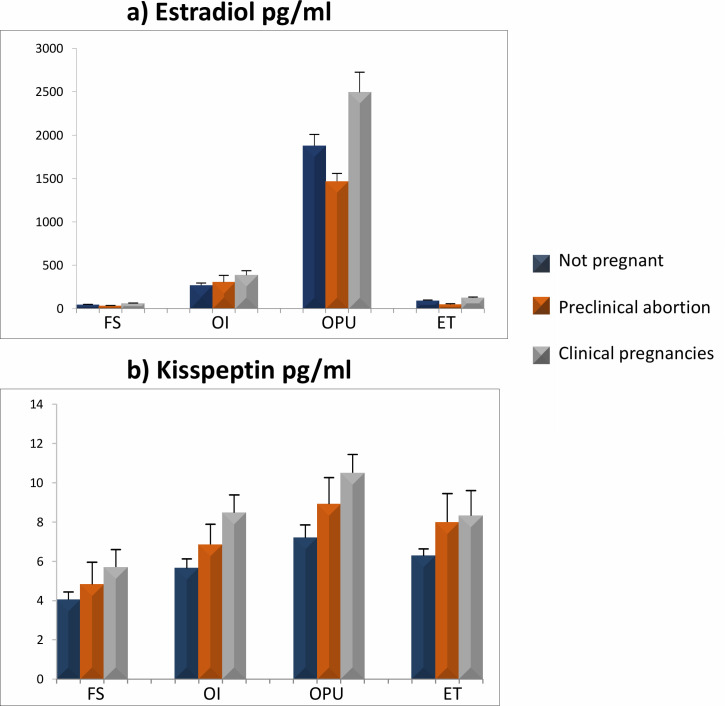
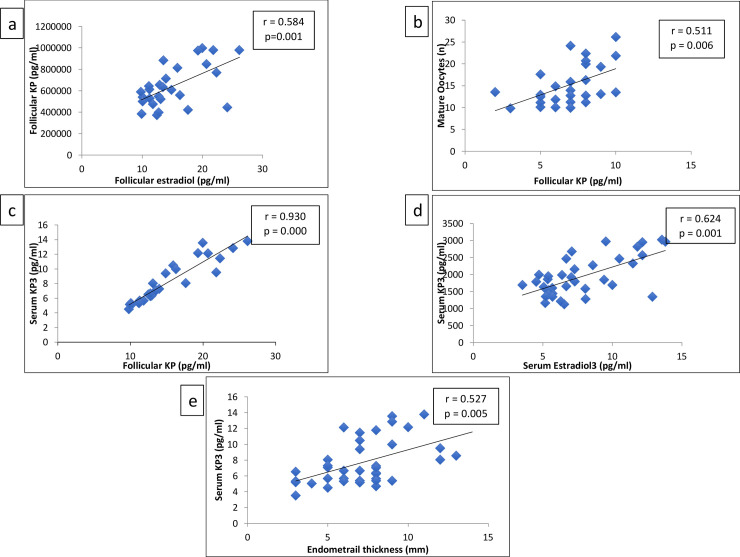
Results: The age of the study subjects was 32.04 ± 2.29 (Mean±SD) years, with mean BMI of 28.51 ± 4.15 (Mean±SD) kg/m2. Mean serum kisspeptin and estradiol levels increased in all subjects as the stimulation proceeded stages 1-3; however, the mean dropped after retrieval of the oocytes (stage 4). Out of 27 female subjects who completed the cycle, 17 remained non-pregnant, 4 had preclinical abortion, and 6 acquired clinical pregnancy. The FF kisspeptin concentration was significantly higher than serum concentrations and positively correlated with serum and FF estradiol concentrations. FF-kisspeptin correlated with serum kisspeptin in Stage 3 (r = 0.930, p<0.001), maturity of oocyte (r = 0.511, p = 0.006) and endometrial thickness (r = 0.522, p = 0.005). Kisspeptin in stage 3 was also found to correlate with endometrial thickness (r = 0.527, p = 0.005) and with estradiol (r = 0.624, p = 0.001) independently.
Conclusion: Increase in serum and FF-kisspeptin and estradiol levels from stages 1 to 3, resulted in an optimum endometrial thickness, probability of fertilization of oocytes and chances of clinical pregnancy in Assisted Reproductive Techniques /ICSI cycles of unexplained infertile females.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Trevisan CM, Montagna E, de Oliveira R, Christofolini DM, Barbosa CP, Crandall KA, et al. Kisspeptin/GPR54 System: What Do We Know About Its Role in Human Reproduction? Cellular physiology and biochemistry: international journal of experimental cellular physiology, biochemistry, and pharmacology. 2018;49(4):1259–76. 10.1159/000493406 - DOI - PubMed
-
- Gaytan F, Gaytan M, Castellano JM, Romero M, Roa J, Aparicio B, et al. KiSS-1 in the mammalian ovary: distribution of kisspeptin in human and marmoset and alterations in KiSS-1 mRNA levels in a rat model of ovulatory dysfunction. American journal of physiology Endocrinology and metabolism. 2009;296(3):E520–31. 10.1152/ajpendo.90895.2008 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
