

Therapeutic Exercise Approaches to Nonoperative and Postoperative Management of Femoroacetabular Impingement Syndrome
- PMID: 33112956
- PMCID: PMC7863596
- DOI: 10.4085/1062-6050-0488.19
Therapeutic Exercise Approaches to Nonoperative and Postoperative Management of Femoroacetabular Impingement Syndrome
Abstract
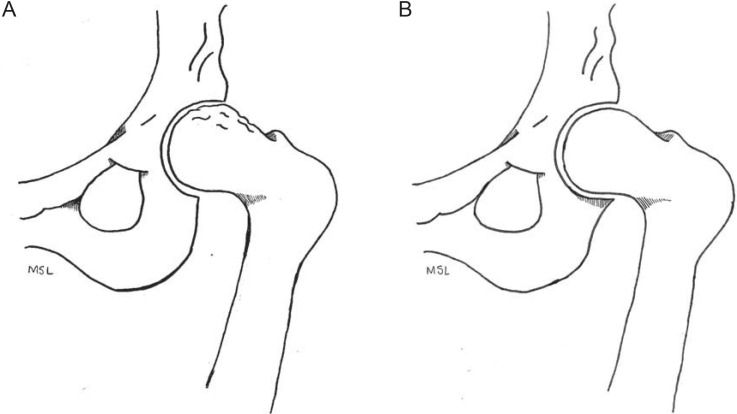
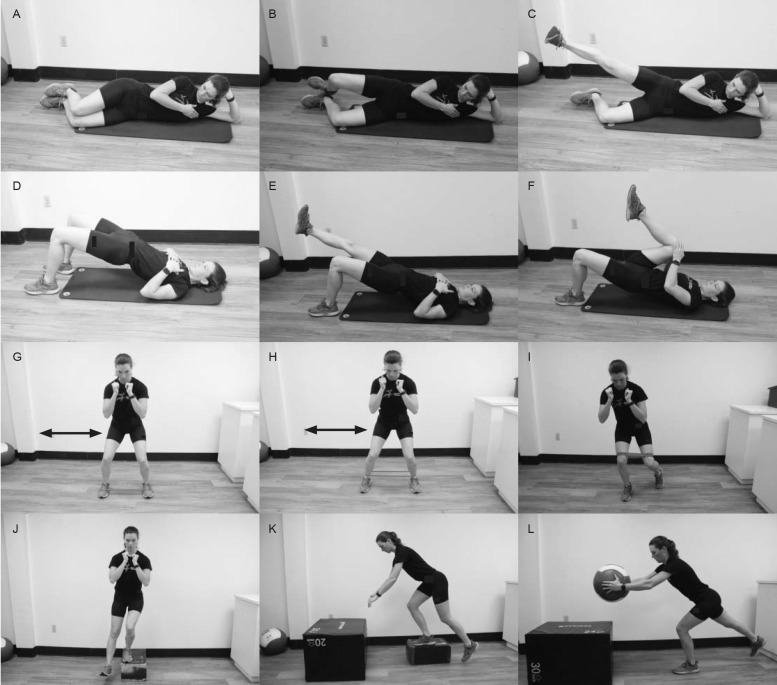
Femoroacetabular impingement syndrome (FAIS) is characterized by premature contact of the femur and acetabulum during hip motion. Morphologic variations of FAIS present as either aspherical femoral deformity (cam femoroacetabular impingement) or overcoverage (pincer femoroacetabular impingement) or both. Patients with FAIS often describe discomfort with hip flexion, adduction, and internal rotation. The use of hip arthroscopy to treat FAIS has risen substantially over the last 15 years. Given that one practice domain of the athletic training profession involves injury prevention and wellness protection, optimal FAIS treatment and management strategies warrant discussion. Sports medicine professionals often help patients with FAIS explore nonoperative exercise strategies and direct rehabilitation exercises for those who pursue surgery. Both approaches demonstrate key pillars of exercise program design, which include postural control, core stabilization, hip strength and motor control, and mobility. The purpose of this article is 2-fold: to present an overview of FAIS, including common diagnostic strategies, and commonalities in therapeutic approaches between nonoperative and postoperative rehabilitation for the treatment and management of patients with FAIS.
Keywords: cam impingement; hip arthroscopy; hip physical examination; hip rehabilitation; pincer deformity.
© by the National Athletic Trainers' Association, Inc.
Figures





References
MeSH terms
LinkOut - more resources
Full Text Sources
